ECB 605 C
Population Studies – II
Semester – VI
Population Census in India and The Salient features of 2011
What is the census?
Census is nothing but a process of collecting, compiling, analyzing, evaluating, publishing and disseminating statistical data regarding the population. It covers demographic, social and economic data and are provided as of a particular date.
When was the first census in India held?
Census operations started in India long back during the period of the Maurya dynasty. It was systematized during the years 1865 to 1872, though it has been conducted uninterruptedly from the year 1881 being a trustworthy resource of information.
Why is the census important?
1. The Indian Census is the most credible source of information on Demography (Population characteristics), Economic Activity, Literacy and Education, Housing & Household Amenities, Urbanisation, Fertility and Mortality, Scheduled Castes and Scheduled Tribes, Language, Religion, Migration, Disability and many other socio-cultural and demographic data since 1872. Census 2011 is the 15th National Census of the Country. This is the only source of primary data in the village , town and ward level, It provides valuable information for planning and formulation policies for Central and the State Governments and is widely used by National and International Agencies, scholars, business people, industrialists, and many more.
2. The delimitation/reservation of Constituencies – Parliamentary/Assembly/Panchayats and other Local Bodies is also done on the basis of the demographic data thrown up by the Census. Census is the basis for reviewing the country’s progress in the past decade, monitoring the ongoing Schemes of the Government and most importantly, plan for the future.
Key findings of 2011 census
1. Population –
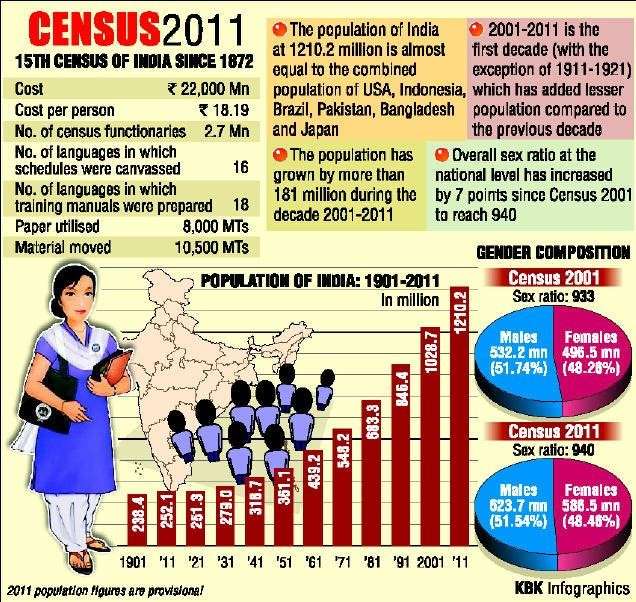
- India’s total population stands at 1.21 billion, which is 17.7 per cent more than the last decade, and growth of females was higher than that of males.
- There was an increase of 90.97 million males and increase of 90.99 million females. The growth rate of females was 18.3 per cent which is higher than males — 17.1 per cent. India’s population grew by 17.7 per cent during 2001-11, against 21.5 per cent in the previous decade.
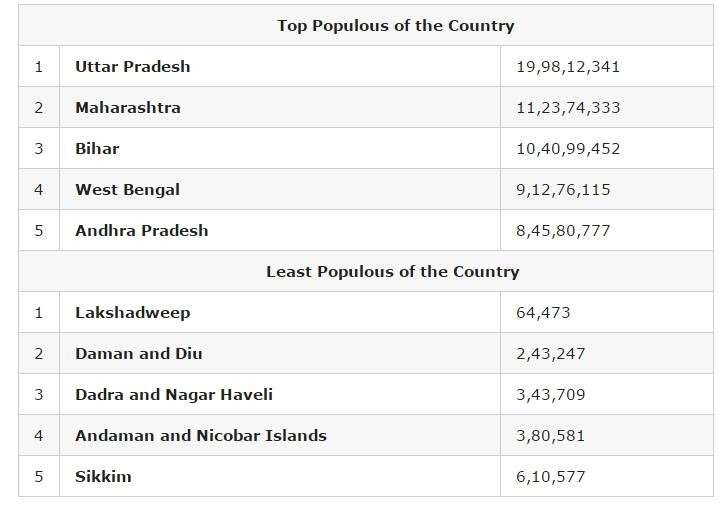
- Among the major states, highest decadal growth in population has been recorded in Bihar (25.4 per cent) while 14 states and Union Territories have recorded population growth above 20 per cent.

2. Rural and urban population –
- Altogether, 833.5 million persons live in rural area as per Census 2011, which was more than two-third of the total population, while 377.1 million persons live in urban areas. Urban proportion has gone up from 17.3 per cent in 1951 to 31.2 per cent in 2011. Empowered Action Group (EAG) states have lower urban proportion (21.1 per cent) in comparison to non-EAG states (39.7 per cent).
- Highest proportion of urban population is in NCT Delhi (97.5 per cent). Top five states in share of urban population are Goa (62.2 per cent), Mizoram (52.1 per cent), Tamil Nadu (48.4 per cent), Kerala (47.7 per cent) and Maharashtra (45.2 per cent).
3. Literacy –
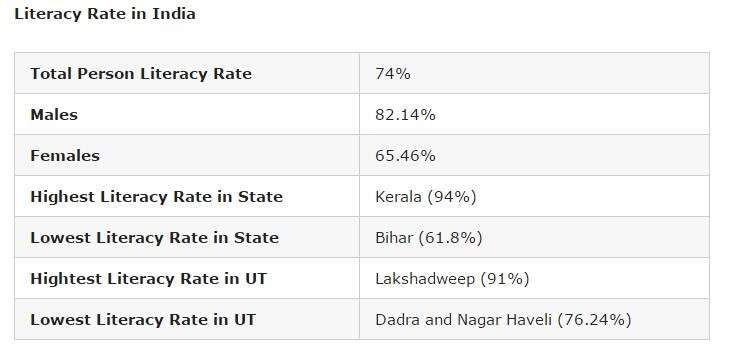
- Literacy rate in India in 2011 has increased by 8 per cent to 73 per cent in comparison to 64.8 per cent in 2001.
- While male literacy rate stands at 80.9 per cent – which is 5.6 per cent more than the previous census, the female literacy rate stands at 64.6 per cent — an increase of 10.9 per cent than 2001.
- The highest increase took place in Dadra and Nagar Haveli by 18.6 points (from 57.6 per cent to 76.2 per cent), Bihar by 14.8 points (from 47.0 per cent to 61.8 per cent), Tripura by 14.0 points (from 73.2 per cent to 87.2 per cent)
- Improvement in female literacy is higher than males in all states and UTs, except Mizoram (where it is same in both males and females) during 2001-11.
- The gap between literacy rate in urban and rural areas is steadily declining in every census. Gender gap in literacy rate is steadily declining in every census. In Census 2011, the gap stands at 16.3 points.
- Top five states and UTs, where literacy rate is the highest, are Kerala (94 per cent), Lakshadweep (91.8 per cent), Mizoram (91.3 per cent), Goa (88.7 per cent) and Tripura (87.2).
- The bottom five states and UTs are Bihar (61.8 per cent), Arunachal Pradesh (65.4 per cent), Rajasthan (66.1 per cent), Jharkhand (66.4 per cent) and Andhra Pradesh (67 per cent).
4. Density –
- The density of population in the country has also increased from 325 in 2001 to 382 in 2011 in per sq km. Among the major states, Bihar occupies the first position with a density of 1106, surpassing West Bengal which occupied the first position during 2001.
- Delhi (11,320) turns out to be the most densely inhabited followed by Chandigarh (9,258), among all states and UT’s, both in 2001 and 2011 Census. The minimum population density works out in Arunachal Pradesh (17) for both 2001 and 2011 Census.
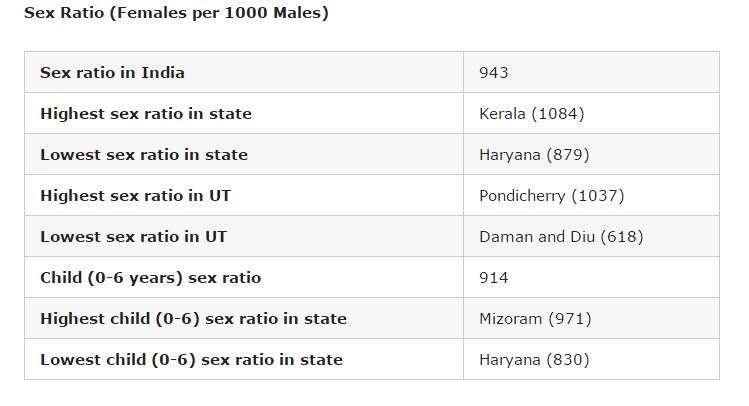
5. Sex ratio –
- The sex ratio of population in the country in 2011 stands at 940 female against 1000 males, which is 10 per cent more than the last census when the number female per thousand male stood at 933. Haryana has the dubious distinction of having the worst male-female ratio among all states while Kerala fares the best.
- The number of females per 1000 males in Haryana in 2011 stands at 879 followed by Jammu and Kashmir (889 female) and Punjab (895 females).
- The other two worst-performing states in terms of skewed sex ration are Uttar Pradesh (912 females) and Bihar (918 females).
- Five top performing states in terms of sex ratio were Kerala (1,084 females), Tamil Nadu (996), Andhra Pradesh (993), Chhattisgarh (991), Odisha (979).
6. Child population –
- Child population in the age of 0 to 6 years has seen an increase of 0.4 per cent to 164.5 million in 2011 from 163.8 million in 2001.
- The child population (0-6) is almost stationary. In 17 states and UTs, the child population has declined in 2011 compared to 2001.
- With the declaration of sex ratio in the age group 0-6, the Census authorities tried to bring out the recent changes in the society in its attitude and outlook towards the girl child. It was also an indicator of the likely future trends of sex ratio in the population.
- There has been a decline of 8 per cent in the sex ratio of 0-6 age group. In 2011, the child sex ratio (0-6) stands at 919 female against 1000 male in comparison to 927 females in 2001.
- Male child (0-6) population has increased whereas female child population has decreased during 2001-11. Eight states, Jammu and Kashmir, Rajasthan, Uttar Pradesh, Bihar, Jharkhand, Arunachal Pradesh, Mizoram, and Meghalaya have proportion of child population more than 15 per cent.
- The worst performing states in regard to sex ration in the age group of 0 to 6 years are Haryana (834 females), Punjab (846), Jammu and Kashmir (862), Rajasthan (888) and Gujarat (890).
- The best performing states are Chhattisgarh (969), Kerala (964), Assam (962), West Bengal (956) Jharkhand (948) and Karnataka (948).
7. SC/ST data –
- According to the Census, Scheduled Castes are notified in 31 states and UTs and Scheduled Tribes in 30 states. There are altogether 1,241 individual ethnic groups, etc. notified as SC’s in different states and UT’s.
- The number of individual ethnic groups, etc. notified as ST’s is 705. There has been some changes in the list of SC’s/ST’s in states and UT’s during the last decade.
- The SC population in India now stands at 201.4 million, which is 20 per cent more than the last census. The ST population stands at 104.3 million in 2011 – 23.7 per cent more than 2001.
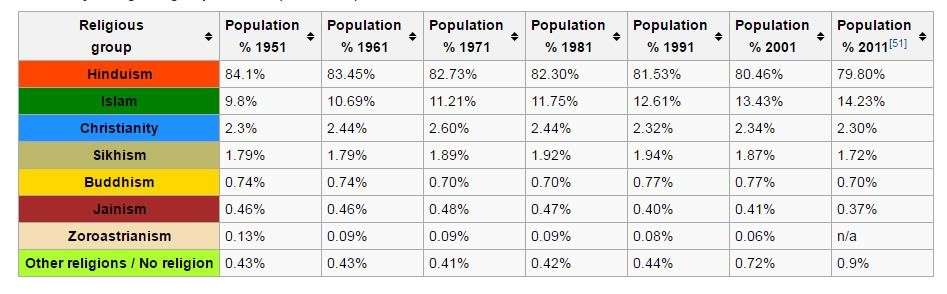
8. Religious demographics – The religious data on India Census 2011 was released by the Government of India on 25 August 2015. Hindus are 79.8% (966.3 million), while Muslims are 14.23% (172.2 million) in India. For the first time, a “No religion” category was added in the 2011 census. 2.87 million Were classified as people belonging to “No Religion” in India in the 2011 census. – 0.24% of India’s population of 1.21 billion. Given below is the decade-by-decade religious composition of India till the 2011 census. There are six religions in India that have been awarded “National Minority” status – Muslims, Christians, Sikhs, Jains, Buddhists and Parsis.
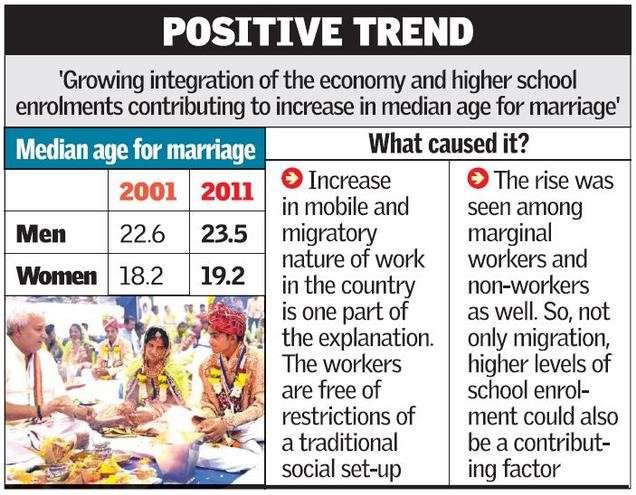
9. Median marriage age – The median age increased for men – from 22.6 (2001) to 23.5 (2011) and for women – from 18.2 (2001) to 19.2 (2011)
The salient features of census 2011
The most important feature of the data contained in Census 2011 and 2001 is that in terms of demographics the Hindus of India are a civilization in retreat. On the other hand Islam is in a fast forward mode. A projection of the future demographics of Hindus and Muslims upto 2050 by Pew Research Center of USA says that upto 2050 worldwide the Hindus will grow at the rate of 34 percent per decade, while Muslims will grow at the rate of 73 percent per decade. A demographically growing community tries to snatch more land, more jobs, more resources and finally demands a major say in the affairs of the besieged country. According to Samuel Huntington it leads to major faultline conflicts between the demographically retreating community and the demographically growing community. In terms of Huntington’s analysis a major civilizational clash between the retreating and advancing communities is inevitable.
The new challenge for Census 2021
Amid the anger and acrimony over the Citizenship Amendment Act (CAA), the National Population Register (NPR), and a possible National Register of Citizens (NRC), which the government has said has not been finalised yet, there has been little thought regarding its effects on another growing challenge — the quality of official data. In the last few years, official data has suffered from credibility issues and undermined confidence in the economy. The Indian statistical system, once the envy of the developing world, has fallen on hard times.
In 2020 and 2021, the government will roll out the 16th Census (and the 8th after Independence). The Census will be conducted in two phases — a house listing and housing Census to be conducted between April and September this year, followed by the population enumeration in February 2021.
The Census is the key source of primary data at the village, town and ward level, providing micro-level data on demography, housing, assets, education, economic activity, social groups, language and migration, among other variables. It also provides population data to the Delimitation Commission for the constitutionally-mandated decennial delimitation of parliamentary and assembly constituencies, and serves as a key input for many government policies and public services.
It is a massive exercise — and massively expensive. The cost of the 2021 Census is estimated at ~8,754 crore (and NPR at ~3,941 crore), involving about 30 lakh enumerators and field functionaries (generally government teachers and those appointed by state governments). Concurrently, the NPR — first prepared in 2010 under the provisions of the Citizenship Act, 1955 and Citizenship Rules, 2003 and subsequently updated in 2015 — will also be updated along with house listing and housing Census (except in Assam).
News reports have been streaming in that data collection exercises like the National Sample Survey (NSS) are being hampered in states like Andhra Pradesh and West Bengal. Reports from Karnataka indicate that people are declining to share personal information with officials visiting households in connection with government welfare schemes, with residents turning away ASHA workers on a pulse-polio visit, fearing that somehow some of their information might find its way into the NRC.
At its core, the fears of a tainted Census stem from the NPR breaking one of the cardinal rules in objective data collection, the preservation of anonymity. Anonymity must be maintained if people are to report information truthfully, especially information that can be used against them. Otherwise, people will report the information that is most likely to yield a beneficial outcome, whether minimising risk or maximising benefits, not what is true.
If respondents ascertain that truthfully revealing certain kinds of information in the NPR is more likely to result in questioning their citizenship, they may choose to obfuscate or misreport. Because the NPR and Census are to be run concurrently — and both are under the auspices of the Registrar General of the ministry of home affairs (also the key architect and driver of the CAA) — this loss of credible information is likely to extend to the Census. Thus, if the CAA and NPR are perceived as targeting a particular community, measuring that community, however genuine the intentions, through the Census, will simply not work.
Given that those born after July 1987 will have to offer proof of their parents’ citizenship, and some segments of citizens, especially Muslims, are particularly vulnerable to having their citizenship questioned, there will be considerable incentives for people to misreport age, religion and language data. But once the trust is broken between the person collecting the data and the person providing the data, then misreporting could spread to other parts of the Census as well. Worse yet, there is no objective way to detect this misreporting, leaving only ad hoc methods of rooting out misreporting that are bound to cause more harm than good.
The loss of credible Census data is an example of an economic principle known as Goodhart’s Law, which states that ‘‘as soon as a particular instrument or asset is publicly defined as money in order to impose monetary control, it will cease to be used as money and replaced by substitutes which will enable evasion of that control’’. In other words, when the measure becomes a target, it ceases to be a good measure. More broadly, measures that are targets simultaneously describe and prescribe, conflating the “what” with the “ought”.
The Census data is, by definition, a means to serve government goals. Assurances of data protection and integrity are unlikely to allay fears that the data gathered will not be used for citizenship purposes. Entire censuses have been stopped in countries such as Lebanon, Nigeria, and Pakistan because of fears that the results would favour certain groups, and led to the pulling out of the citizenship question in the 2020 US Census.
Sadly, the negative repercussions go beyond the Census. For example, good quality personal information is critical for many public health programmes. Incomplete data can have serious adverse effects on monitoring and evaluation, and, thereby programme outcomes. Indeed, surveys, in general, will be negatively affected since once distrust takes root, it becomes a generalised condition.
The compact between a State and its citizens is built on a foundation of trust, one that is based on a minimal presumption that people are citizens of that State to begin with. The erosion of that trust will undermine the Indian State’s ability to gather credible data. And a State that cannot collect objective data on its population will also find itself incapable of framing effective policies for its people.
National Family Health Survey 3, 4 & 5
- National Family Health Survey (NFHS):
- The NFHS is a large-scale, multi-round survey conducted in a representative sample of households throughout India.
- Conducted By:
- The Ministry of Health and Family Welfare (MoHFW) has designated the International Institute for Population Sciences(IIPS) Mumbai, as the nodal agency for providing coordination and technical guidance for the survey.
- IIPS collaborates with a number of Field Organizations (FO) for survey implementation.
- Goals:
- Each successive round of the NFHS has had two specific goals:
- To provide essential data on health and family welfare needed by the Ministry of Health and Family Welfare and other agencies for policy and programme purposes.
- To provide information on important emerging health and family welfare issues.
- Each successive round of the NFHS has had two specific goals:
- The survey provides state and national information for India on:
- Fertility
- Infant and child mortality
- The practice of family planning
- Maternal and child health
- Reproductive health
- Nutrition
- Anaemia
- Utilization and quality of health and family planning services.
- Funding:
- The funding for different rounds of NFHS has been provided by USAID, the Bill and Melinda Gates Foundation, UNICEF, UNFPA, and MoHFW (Government of India).
History of NFHS
- Objective: The main objective of each successive round of the NFHS has been to provide high-quality data on health and family welfare and emerging issues in this area.
- NFHS-1: The NFHS-1 was conducted in 1992-93.
- NFHS-2: The NFHS-2 was conducted in 1998-99 in all 26 states of India.
- The project was funded by the USAID, with additional support from UNICEF.
- NFHS-3: The NFHS-3 was carried out in 2005-2006.
- NFHS-3 funding was provided by the USAID, the Department for International Development (UK), the Bill and Melinda Gates Foundation, UNICEF, UNFPA, and the Government of India.
- NFHS-4: The NFHS-4 in 2014-2015.
- In addition to the 29 states, NFHS-4 included all six union territories for the first time and provided estimates of most indicators at the district level for all 640 districts in the country as per the 2011 census.
- The survey covered a range of health-related issues, including fertility, infant and child mortality, maternal and child health, perinatal mortality, adolescent reproductive health, high-risk sexual behaviour, safe injections, tuberculosis, and malaria, non-communicable diseases, domestic violence, HIV knowledge, and attitudes toward people living with HIV.
National Family Health Survey-5
- The NFHS-5 has captured the data during 2019-20 and has been conducted in around 6.1 lakh households.
- Many indicators of NFHS-5 are similar to those of NFHS-4, carried out in 2015-16 to make possible comparisons over time.
- Phase 2 of the survey (covering remaining states) was delayed due to the Covid-19 pandemic and its results were released in September 2021.
- NFHS-5 data will be useful in setting benchmarks and examining the progress the health sector has made over time.
- Besides providing evidence for the effectiveness of ongoing programmes, the data from NFHS-5 help in identifying the need for new programmes with an area specific focus and identifying groups that are most in need of essential services.
- It provides an indicator for tracking 30 Sustainable Development Goals (SDGs) that the country aims to achieve by 2030.
- NFHS-5 includes some new topics, such as preschool education, disability, access to a toilet facility, death registration, bathing practices during menstruation, and methods and reasons for abortion.
- NFHS-5 includes new focal areas that will give requisite input for strengthening existing programmes and evolving new strategies for policy intervention. The areas are:
- Expanded domains of child immunization
- Components of micro-nutrients to children
- Menstrual hygiene
- Frequency of alcohol and tobacco use
- Additional components of non-communicable diseases (NCDs)
- Expanded age ranges for measuring hypertension and diabetes among all aged 15 years and above.
- In 2019, for the first time, the NFHS-5 sought details on the percentage of women and men who have ever used the Internet.
- NFHS-5 includes new focal areas that will give requisite input for strengthening existing programmes and evolving new strategies for policy intervention. The areas are:
Key Findings of NFHS-5
- Sex Ratio: NFHS-5 data shows that there were 1,020 women for 1000 men in the country in 2019-2021.
- This is the highest sex ratio for any NFHS survey as well as since the first modern synchronous census conducted in 1881.
- In the 2005-06 NFHS, the sex ratio was 1,000 or women and men were equal in number.
- Sex Ratio at Birth: For the first time in India, between 2019-21, there were 1,020 adult women per 1,000 men.
- However, the data shall not undermine the fact that India still has a sex ratio at birth (SRB) more skewed towards boys than the natural SRB (which is 952 girls per 1000 boys).
- Uttar Pradesh, Haryana, Punjab, Rajasthan, Bihar, Delhi, Jharkhand, Andhra Pradesh, Tamil Nadu, Odisha, Maharashtra are the major states with low SRB.
- Total Fertility Rate (TFR): The TFR has also come down below the threshold at which the population is expected to replace itself from one generation to next.
- TFR was 2 in 2019-2021, just below the replacement fertility rate of 2.1.
- In rural areas, the TFR is still 2.1.
- In urban areas, TFR had gone below the replacement fertility rate in the 2015-16 NFHS itself.
- A decline in TFR, which implies that a lower number of children are being born, also entails that India’s population would become older.
- The survey shows that the share of under-15 population in the country has therefore further declined from 28.6% in 2015-16 to 26.5% in 2019-21.
- TFR was 2 in 2019-2021, just below the replacement fertility rate of 2.1.
- Children’s Nutrition: Child Nutrition indicators show a slight improvement at all-India level as Stunting has declined from 38% to 36%, wasting from 21% to 19% and underweight from 36% to 32% at all India level.
- In all phase-II States/UTs the situation has improved in respect of child nutrition but the change is not significant as drastic changes in respect of these indicators are unlikely in a short span period.
- The share of overweight children has increased from 2.1% to 3.4%.
- In all phase-II States/UTs the situation has improved in respect of child nutrition but the change is not significant as drastic changes in respect of these indicators are unlikely in a short span period.
- Anaemia: The incidence of anaemia in under-5 children (from 58.6 to 67%), women (53.1 to 57%) and men (22.7 to 25%) has worsened in all States of India (20%-40% incidence is considered moderate).
- Barring Kerala (at 39.4%), all States are in the “severe” category.
- Immunization: Full immunization drive among children aged 12-23 months has recorded substantial improvement from 62% to 76% at all-India level.
- 11 out of 14 States/UTs have more than three-fourth of children aged 12-23 months with fully immunization and it is highest (90%) for Odisha.
- Institutional Births: Institutional births have increased substantially from 79% to 89% at all-India Level.
- Institutional delivery is 100% in Puducherry and Tamil Nadu and more than 90% in 7 States/UTs out of 12 Phase II States/UTs.
- Along with an increase in institutional births, there has also been a substantial increase in C-section deliveries in many States/UTs especially inprivate health facilities.
- It calls into question unethical practices of private health providers who prioritise monetary gain over women’s health and control over their bodies.
- Family Planning: Overall Contraceptive Prevalence Rate (CPR) has increased substantially from 54% to 67% at all-India level and in almost all Phase-II States/UTswith an exception of Punjab.
- Use of modern methods of contraceptives has also increased in almost all States/UTs.
- Unmet needs of family Planning have witnessed a significant decline from13% to 9% at all-India level and in most of the Phase-II States/UTs.
- The unmet need for spacing which remained a major issue in India in the past has come down to less than 10% in all the States except Jharkhand (12%), Arunachal Pradesh (13%) and Uttar Pradesh(13%).
- Breastfeeding to Children’s: Exclusive breastfeeding to children under age 6 months has shown an improvement in all-India level from 55% in 2015-16 to 64% in 2019-21. All the phase-II States/UTs are also showing considerable progress.
- Women Empowerment: Women’s empowerment indicators portray considerable improvement at all India level and across all the phase-II States/UTs.
- Significant progress has been recorded between NFHS-4 and NFHS-5 in regard to women operating bank accounts from 53% to 79% at all-India level.
- More than 70% of women in every state and UTs in the second phase have operational bank accounts.
Key Terms
- Total Fertility Rate (TFR) indicates the average number of children expected to be born to a woman during her reproductive span of 15-49 years.
- The replacement level is the number of children needed to replace the parents, after accounting for fatalities, skewed sex ratio, infant mortality, etc. Population starts falling below this level.
- Contraceptive Prevalence Rate (CPR) is the proportion of women who are currently using, or whose sexual partner is currently using, at least one method of contraception, regardless of the method being used.
- It is reported as a percentage with reference to women of respective marital status and age group.
- Sex ratio at birth (SRB) is defined as the number of female births per 1,000 male births. The SRB is a key indicator of a son’s preference vis-à-vis daughters.
- Stunting is the impaired growth and development that children experience from poor nutrition, repeated infection, and inadequate psychosocial stimulation.
- It is the result of chronic or recurrent undernutrition, usually associated with poverty, poor maternal health and nutrition, frequent illness and/or inappropriate feeding and care in early life.
- Wasting is defined as low weight-for-height. It often indicates recent and severe weight loss, although it can also persist for a long time. Wasting in children is associated with a higher risk of death if not treated properly.
- Infant Mortality Rate (IMR) is defined as the ‘number of deaths of children under the age of 1 year per 1000 live births for a given year.
- The country’s average IMR stands at 32 per 1,000 live births which includes an average 36 deaths for rural and 23 for urban areas.
Characteristics of Indian population
By demographic features we mean the characteristics of population like, size, composition, diversity, growth and quality of population etc.
To have basic understanding of the population problem of a specific country, one should have a complete knowledge regarding the basic features of population of that country.
The following are features of India’s population:
1. Large Size and Fast Growth:
The first main feature of Indian population is its large size and rapid growth. According to 2001 census, the population of India is 102.87 crore. In terms of size, it is the second largest population in the world, next only to China whose population was 127 crore in 2001. India’s population was 23.6 crore in 1901 and it increased to 102.7 crore in 2001.
In addition to its size, the rate of growth of population has been alarming since 1951. At present, India’s population is growing at a rate of 1.9 percent per annum; 21 million people are added every year which is more than the population of Australia. This situation is called population explosion and this is the result of high birth rate and declining death rate.
2. Second Stage of Demographic Transition:
According to the theory of demographic transition, the population growth of a country passes through three different stages as development proceeds. The first stage is characterised by high birth rate and high death rate. So in this stage the net growth of population is zero. Till 1921, India was in the 1st stage of demographic transition.
The second stage is featured by high birth rate and declining death rate leading to the rapid growth of population. India entered the second stage of demographic transition after 1921. In 1921-30 India entered the 2nd stage, the birth rate was 464 per thousand and death rate was 363 per thousand.
In 2000-01, birth rate was 25.8 and death rate declined to 85. This led to rapid growth of population. India is now passing through the second stage of demographic transition. While developed countries are in 3rd stage.
3. Rapidly Rising Density:
Another feature of India’s population is its rapidly rising density. Density of population means to the average number of people living per square kilometer. The density of population in India was 117 per square km. in 1951 which increased to 324 in 2001. This makes India one of the most densely populated countries of the world. This adversely affects the land-man ratio.
India occupies 2.4 per-cent of the total land area of the world but supports 16.7 per-cent of the total world population. Moreover, there is no causal relationship between density of population and economic development of a country. For example, Japan & England having higher density can be rich and Afghanistan & Myanmar having lower density can be poor. However in an underdeveloped country like India with its low capital and technology, the rapidly rising density is too heavy a burden for the country to bear.
4. Sex Ratio Composition Unfavourable to Female:
Sex ratio refers to the number of females per thousand males. India’s position is quite different than other countries. For example the number of female per thousand males was 1170 in Russia, 1060 in U.K., 1050 in U.S.A. whereas it is 927 in India according to 1991 census.
The sex ratio in India as 972 per thousand in 1901 which declined to 953 in 1921 and to 950 in 1931. Again, in 1951, sex ratio further declined to 946. In 1981, sex ratio reduced to 934 against 930 per thousand in 1971. During 1991, sex ratio was recorded 927 per thousand.
The sex ratio is 933 per thousand in 2001. State wise Kerala has more females than males. There are 1040 females per thousand males. The lowest female ratio was recorded in Sikkim being 832. Among the union territories Andaman and Nicobar Islands has the lowest sex ratio i.e. 760. Therefore, we can conclude that sex ratio composition is totally unfavourable to female.
5. Bottom heavy Age Structure:
The age composition of Indian population is bottom heavy. It implies that ratio of persons in age group 0-14 is relatively high. According to 2001 census, children below 14 years were 35.6%. This figure is lower than the figures of previous year. High birth rate is mainly responsible for large number of dependent children per adult. In developed countries the population of 0-14 age group is between 20 to 25%. To reduce the percentage of this age group, it is essential to slow down the birth rate.
6. Predominance of Rural Population:
Another feature of Indian population is the dominance of rural population. In 1951, rural population was 82.7% and urban population was 17.3%. In 1991 rural population was 74.3% and urban population was 257. In 2001, the rural population was 72.2% and urban population was 27.8. The ratio of rural urban population of a country is an index of the level of industrialisation of that country. So process of urbanisation slow and India continues to be land of villages.
7. Low Quality Population:
The quality of population can be judged from life expectancy, the level of literacy and level of training of people. Keeping these parameters in mind, quality of population in India is low.
(a) Low Literacy Level:
Literacy Level in India is low. Literacy level in 1991 was 52.2% while male-female literacy ratio was 64.1 and 39.3 percent. In 2001, the literacy rate improved to 65.4 percent out of which made literacy was 75.8 and female literacy was 52.1 percent. There are 35 crore people in our country who are still illiterate.
(b) Low level of Education and Training:
The level of education and training is very low in India. So quality of population is poor. The number of persons enrolled for higher education as percentage of population in age group 20-25 was a percent in 1982. It is only one fourth of the developed countries. The number of doctors and engineers per million of population are 13 and 16 respectively. It is quite less as compared to advanced countries.
(c) Low Life Expectancy:
By life expectancy we mean the average number of years a person is expected to live. Life expectancy in India was 33 years. It was increased to 59 in 1991 and in 2001, life expectancy increased to 63.9. Decline in death rate, decline in infant mortality rate and general improvement in medical facilities etc. have improved the life expectancy. However life expectancy is lower in India as compared to life expectancy of the developed nations. Life expectancy is 80 year in Japan and 78 years in Norway.
8. Low Work Participation Rate:
Low proportion of labour force in total population is a striking feature of India’s population. In India, Labour force means that portion of population which belongs to the age group of 15-59. In other words, the ratio of working population to the total is referred to as work participation rate.
This rate is very low in India in comparison to the developed countries of the world. Total working population was 43% in 1961 which declined to 37.6% in 1991. This position improved slightly to 39.2% in 2001. That means total non-working population was 623 million (60.8 percent) and working population was 402 million (39.2%). Similarly low rate of female employment and bottom-heavy age structure are mainly responsible for low work participation in India.
9. Symptoms of Over-population:
The concept of over-population is essentially a quantitative concept. When the population size of the country exceeds the ideal size, we call it over-population. According to T.R. Malthus, the father of demography, when the population of a country exceeds the means of substance available, the country faces the problem of over-population.
No doubt, food production has increased substantially to 212 million tonnes but problems like poverty, hunger, malnutrition are still acute. Agriculture is overcrowded in rural areas of the country which is characterised by diminishing returns. This fact leads to the conclusion that India has symptoms of over-population. Indian low per capita income, low standard of living, wide spread unemployment and under-employment etc. indicate that our population size has crossed the optimum limit.
Birth, Death and Population Growth Rates in India
Introduction
India is the second most populated country in the world. In land area, India ranks seventh globally. The population of India contributes nearly 17.70% share of the world’s population. Uttar Pradesh, Maharashtra and Bihar are India’s top three most populated states. In contrast, Sikkim is the least populated state in the country. At present, China is the most populous country globally, but the birth rate and growth rate of India’s population indicate that India might surpass China’s population in the coming years. Here are some interesting facts about various aspects of India’s demography.
The Birth Rate in India
- As per United Nations International Children’s Emergency Fund (UNICEF), 67,385 babies are born per day in India. This is one-sixth of the total childbirth in the world.
- The annual birth rate in India accounts for one-fifth of the world’s yearly childbirth. Approximately 25 million babies are born per year in India.
- The crude birth rate in India is 17 births per 1000 persons. The natural birth rate is the live births per thousand population in a year, estimated at mid-year.
- By the United Nations (UN) World population prospect, the sex ratio at birth in India is 110 boys for every 100 girls.
- In India, Bihar has the highest birth rate, followed by Uttar Pradesh, Madhya Pradesh and Rajasthan.
- The lowest birth rate in India is reported in Kerala, followed by Punjab, Tamil Nadu and West Bengal.
The Death Rate in India
- The mortality rate or death rate is defined as the number of deaths in a particular population during a specific time.
- According to World Bank’s data, the mortality rate or crude death rate in India is 7.30 per 1000 persons.
- In India, approximately 26789 deaths are reported per day.
- In the 2019 survey, India’s Infant Mortality Rate (IMR) was 30 deaths per 1000 live births.
- In 2019, the female mortality rate was 145.05 per 1000 female adults, and the male mortality rate was 201.4 per 1000 male adults in India.
The Population Growth Rate of India
As per the United Nations (UN) estimates, the population of India in 2022 will be 140 crores, and the present growth rate of the population is 1%. In the past decades, the growth rate of India’s population has significantly declined, but it is still higher than the population growth rate of China. It is estimated that India will surpass China and become the most populated country by 2030. However, after it, the population growth rate will become stagnant and then start to decline. It is expected that the population of India will reach its peak level by 2060 with 1.65 billion people, and then it will begin to decrease.
India is one of the youngest nations in the world. More than 50% of India’s population is below the age of 25, and only 5% of the people of India are above the age of 65 years.
Male and Female Population Statistics of India
As per the fifth National Family and Health Survey (NFHS), the male and female ratio in India is 1020 women for every 1000 men. For the first time in the history of India, it has more women than men. As per the 2015-16 NFHS survey, the ratio was 991 females for every 1000 males.
However, the sex ratio at birth in 2020-21 is 937 female births for every 1000 male births. It still indicates that the problem of sex selection before the birth of the child and female foeticide is still not completely resolved.
The Fertility Rate in India
As per the fifth National Family and Health Survey (NFHS), the fertility rate in India as of 2021 is 2. The highest fertility rate in the country is recorded in Bihar, with three children per woman, followed by Uttar Pradesh, Jharkhand, Madhya Pradesh and Rajasthan.
The Negative Impact of Population Growth on the Country
- It leads to unemployment as there are more job seekers than the job opportunities evolving in the country.
- When the population growth rate is higher than the country’s economic growth rate, it reduces the per capita income, resulting in inflation and poverty.
- The rise in population results in a vicious circle of unemployment, poverty and illiteracy.
Conclusion
India occupies only 2.14% of the world’s land area, but in terms of the population, its share is 18% of the world’s population. India is among the youngest nations, with a majority population of fewer than 35 years of age. India can emerge as one of the strongest and most developed nations. It is vital to act on necessary measures to realise the true potential of the young Indians. India is a versatile country with more than two thousand ethnic groups. It is important to lower the growth rate of the population to maintain a balanced approach toward the sustainable development of the country.
Life Expectancy
- India’s life expectancy at birth inched up to 69.7 in the 2015-19 period, well below the estimated global average life expectancy of 72.6 years.
- It has taken almost ten years to add two years to life expectancy.
Major Points
- Data shows that the gap between life expectancy at birth and life expectancy at age one or age five is the biggest in states with the highest infant mortality (IMR), Madhya Pradesh and Uttar Pradesh.
- In Uttar Pradesh, with the second highest IMR of 38, life expectancy jumps the highest, by 3.4 years, on completion of the first year.
- Over a 45-year period, India had added about 20 years to its life expectancy at birth from 49.7 in 1970-75 to 69.7 by 2015-19.
- Odisha has had the highest increase, of over 24 years, from 45.7 to 69.8 years followed by Tamil Nadu, where it increased from 49.6 to 72.6.
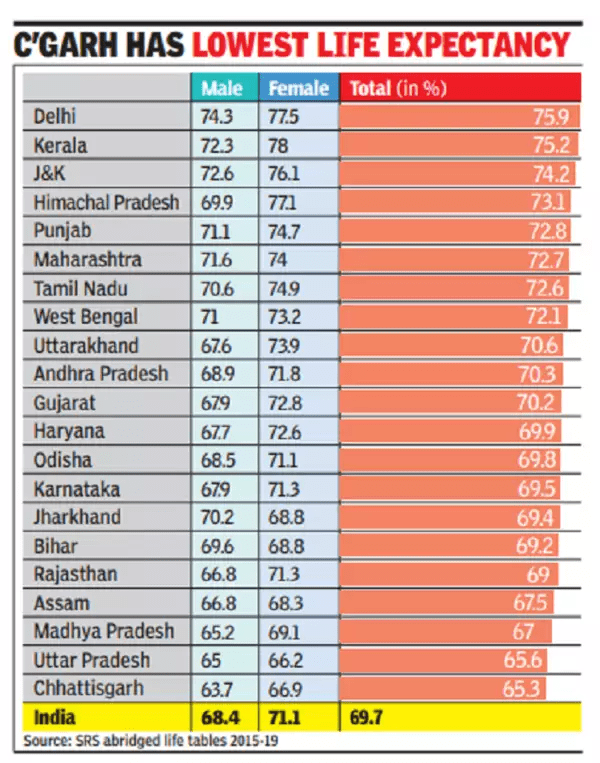
- Within India, there are huge variations across states and between urban and rural areas.
- Urban women in Himachal Pradesh had the highest life expectancy at birth of 82.3 years while at the other end, rural men in Chhattisgarh had the lowest, just 62.8 years, a gap of 15.8 years.
- Comparison with neighbouring countries
- In the neighbourhood, Bangladesh and Nepal, which had lower IMRs than India (24 compared to 28), now have higher life expectancy at birth of 72.1 and 70.5 respectively, according to the UN’s Human Development Report, 2019.
- Japan has the highest life expectancy of 85. Norway, Australia, Switzerland and Iceland had a life expectancy of 83. The Central African Republic had the lowest life expectancy of 54 followed by Lesotho and Chad at 55 in 2020.
Life Expectancy
- It is an estimate of the average number of additional years that a person of a given age can expect to live.
- The most common measure of life expectancy is life expectancy at birth.
- Life expectancy is a hypothetical measure.
- It assumes that the age-specific death rates for the year in question will apply throughout the lifetime of individuals born in that year.
- The estimate, in effect, projects the age-specific mortality (death) rates for a given period over the entire lifetime of the population born (or alive) during that time.
- The measure differs considerably by sex, age, race, and geographic location.
- Therefore, life expectancy is commonly given for specific categories, rather than for the population in general. For example, the life expectancy for white females in the United States who were born in 2003 is 80.4 years.
Infant and Maternal Mortality Rate in India
Infant Mortality Rate:
The Infant Mortality Rate or IMR is the number of deaths of children (under one year of age) per 1000 live births. On the other hand, the death rate of children under five year of age is called Child Mortality Rate.
Infant Mortality Rate
According to data presented by the Census of India – “The infant mortality rate, which plays an important role in health planning, has shown a considerable decline from 129 per 1000 live births in 1971 to 110 in 1981 and from 80 in 1991 to 33 in 2017.”
- This rate for a region is calculated by dividing the number of deaths of children less than 1 year old by the number of live births in a year times 1000.
- The major causes of congenital infant mortality are sudden infant death syndrome, malformations, accidents, maternal complications during the pregnancy and unintentional injuries.
- Contributing causes are social and environmental obstacles that prevent the availability of basic medical resources. 99% of the deaths of infants take place in developing nations. Among these, 86% are caused due to premature births, infections, delivery complications, birth injuries and perinatal asphyxia.
Infant Mortality Rate in India
- AS per Census 2011, The infant mortality rate, which plays an important role in health planning, has shown a considerable decline from 129 per 1000 live births in 1971 to 110 in 1981 and from 80 in 1991 to 44 in 2011. The child mortality rate has depicted a perceptible decline from 51.9 in 1971 to 41.2 in 1981 and from 26.5 in 1991 to 12.2 in 2011.
- Also, World Bank has indicated 28.3 as Infant Mortality Rate of India for 2019.
- According to the latest sample registration system Bulletin, Infant Mortality Rate in Kerala – 7 (updated)
- Infant Mortality Rate in Madhya Pradesh – 48 (updated)
- In India, Nagaland has the best Infant Mortality Rate which is at 4.
- As per RBI, the Infant Mortality Rate of the National Capital Delhi is 13.
- The infant mortality rate among females is higher than among males in all Indian states except:
- Chhattisgarh
- Delhi
- Madhya Pradesh
- Tamil Nadu
- Uttarakhand
Note: The 32 is the IMR at the national level. The rate varies between 6.9 and 5.0 in urban areas and rural areas respectively.
Replacement Rate
- In the case of no female mortality until the culmination of childbearing age (44/45/49), the replacement level of the TFR would be quite near 2.
- The current India Total Fertility Rate is 2.2 (2020).
- The lowest TFR 2019-2020 as per National Family Health Survey 5 is recorded in Sikkim (1.1). Bihar has the highest TFR – 3 (in 2005-06 the TFR was 4).
- According to the latest National Family Health Survey (NFHS), the TFR across most Indian states declined in the past half a decade, more so among urban women.
- The fertility rate of women in rural areas sharply dropped in Jammu and Kashmir, Maharashtra, Assam, Nagaland, Manipur, Mizoram, and Bihar, while the fertility rate of women in urban areas went below-replacement fertility across all 21 states except Bihar, where it has remained unchanged at 2.4 since 2015-16.
Maternal Mortality Rate:
Maternal Mortality Rate (MMR) is defined as the number of maternal deaths per 100,000 live births due to pregnancy or termination of pregnancy, regardless of the site or duration of pregnancy. The maternal mortality rate is used to represent the risk associated with pregnancy among women.
In developing countries, the leading cause of death and disability among women of reproductive age are the complications that occur during childbirth and pregnancy.
Maternal Mortality Rate in India
In India, the number of deaths caused due to pregnancy and childbirth has been very high over the years but recent records show that there has been a decline in the MMR of India. It is tough to calculate the exact maternal mortality except where the comprehensive records of deaths and causes of death are available. So surveys and census are used to estimate the levels of maternal mortality.
Reproductive Age Mortality Studies (RAMOS) is presently considered the best way to calculate MMR. In this, different sources and records are analysed to get data regarding the death of women of reproductive ages and also through verbal autopsy to estimate the number of deaths. The MMR is calculated at both global and regional level every five years through a regression model.
In India, the Sample Registration Survey (SRS) is used to get an estimate of the maternal mortality rate. The Office of the Registrar General’s Sample Registration System (SRS) has released a special bulletin on Maternal Mortality in India in March 2022.
Major observations as per the Survey –
- As per the special bulletin there has been a decline of 10 points in the maternal mortality rate of India. India’s maternal mortality ratio (MMR) has improved to 103 in 2017-19, from 113 in 2016-18, marking an 8.8% decline.
- This is in sync with the trend of progressive reduction in the MMR over the years. With this persistent decline, India is on the verge of achieving the National Health Policy (NHP) target of 100/lakh live births by 2020 and certainly on track to achieve the Sustainable Development Goal (SDG) target of 70/ lakh live births by 2030
- Currently seven states have achieved the Sustainable Development Goal (3.1) target. This marks an improvement compared to last survey when only five states had reached the target. Currently these states include Kerala (30), Maharashtra (38), Telangana (56), Tamil Nadu (58), Andhra Pradesh (58), Jharkhand (61), and Gujarat (70).
- Currently there are nine States that have achieved the MMR target set by the National Health Policy. This includes the above seven states along with Karnataka (83) and Haryana (96).
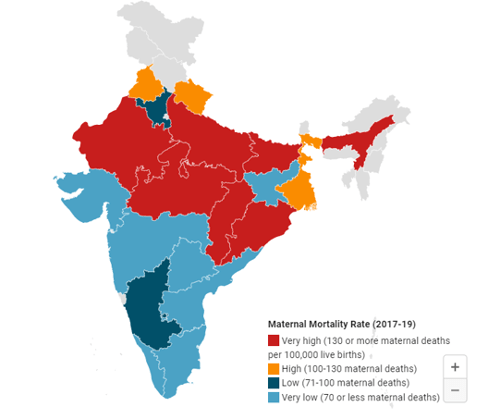
- Despite an improvement in the national average, some states continue to witness high levels of maternal mortality rates.
| Definition | States | |
| Very high maternal mortality | 130 or more maternal deaths per 100,000 live births. | Bihar (130), Odisha (136), Rajasthan (141), Chhattisgarh (160), Madhya Pradesh (163), Uttar Pradesh (167) and Assam (205). |
| High maternal mortality: | 100-130 maternal deaths per 100,000 live births. | Uttarakhand (101), West Bengal (109) and Punjab (114). |
| Low maternal mortality: | 71-100 maternal deaths per 100,000 live births. | Karnataka (83) and Haryana (96). |
- The states of Uttar Pradesh, Rajasthan and Bihar have seen the most drop in MMR in absolute numbers. These states continue to have high level MMRs despite the improvement.
- Uttar Pradesh reported a decline of 30 points, Rajasthan (23 points) and Bihar (19 points).
- A remarkable fall of more than 15 percent has been observed in the states of Kerala, Maharashtra and Uttar Pradesh.
- The top state with the lowest MMR is Kerala while the state with the highest MMR is Assam.
- Notably states like West Bengal, Haryana, Uttarakhand and Chhattisgarh have recorded an increase in MMR over the last survey in contrast to the national trend.
Given below is the MMR in India as per the Sample Registration System:
| Maternal Mortality Rate (MMR) in India | |
| Year | MMR |
| 2004-2006 | 254 |
| 2007-2009 | 212 |
| 2010-2012 | 178 |
| 2011-2013 | 167 |
| 2014-2016 | 130 |
| 2015-2017 | 122 |
| 2016-2018 | 113 |
| 2017-2019 | 103 |
The above data clearly shows the decline in the trend of maternal mortality rate in India. In the survey conducted in 2015-2017, Kerala was the state with the least maternal mortality rate of 42 and Assam noted the maximum number of deaths of women in India with MMR of 229.
Causes of High Maternal Mortality Rate
There are various reasons for the death of women during their reproductive age (18 to 39 years)that had been the cause of an increase in the maternal mortality rate. Given below are a few reasons for the rate of deaths of women due to pregnancy and childbirth:
- Spread of diseases
- Unawareness
- Lack of nutrition and unhealthy livelihood
- Haemorrhage
- Incorrect Treatment
Studies have shown that most deaths during pregnancy and childbirth are curable and can be controlled if proper treatment is provided to women. It has also been noted that calculating the exact MMR is not possible as multiple records of deaths are not recorded for reasons like abortion, ill-treatment and lack of medical attribution.
Result of MDG and SDG with respect to Maternal Mortality Rate
The Millennium Development Goals were set UNDP for all the member nations of the UN. MDG was a set of eight goals that were set for a better future of the world and the people living in it. The Sustainable development goals were undertaken by the members of the UN after a fifteen-year successful plan of the MDG.
The Millennium Development goals were successful in reducing poverty and infant mortality rate almost half since 1990. The latest report of Sustainable development goals released for 2019 has stated that a major decline in the number of deaths caused due to pregnancy and childbirth has been noted across the world.
The report also states that between 2015 and 2018, there has been an increase of 81 per cent assistance provided to pregnant ladies and that has been one of the major reasons for the decline in MMR. In 2018, the report released by SDG stated a decline of 37 per cent in the maternal mortality rate since 2000.
The sustainable development goals intend to attain their target of 70 deaths per 100,000 by 2030 with respect to the maternal mortality rate. Many actions have been taken for a better livelihood and proper assistance is being provided to reproductive women and awareness is being spread with an intention to end the maternal mortality rate across the world.
Maternal Mortality Rate in India – Reasons for Decline
The following programs implemented by the government is playing a crucial role in reducing the Maternal Mortality Rate in India.
Anaemia Mukt Bharat (AMB)
- Anaemia Mukt Bharat (AMB) strategy was launched in 2018 with the objective of reducing anaemia prevalence among children, adolescents and women in the reproductive age group.
- It focusses on six target beneficiary groups, through six interventions and six institutional mechanisms to achieve the envisaged target under the POSHAN Abhiyan.
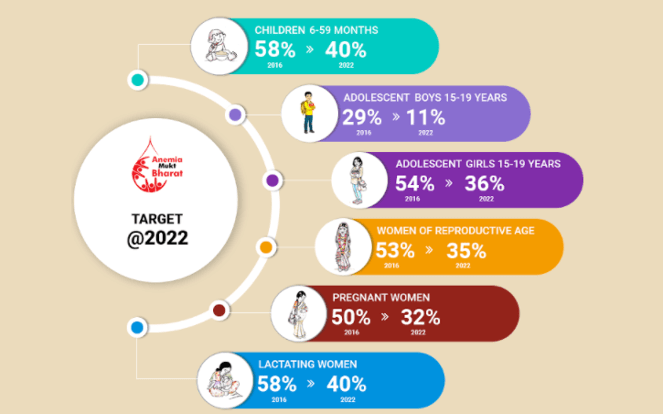
- The 6 interventions include supply of iron and folic acid supplements, deworming, behaviour change communication campaign, testing for anaemia, provision of iron and folic acid fortified foods in government-funded health programmes and addressing of non-nutritional causes of anaemia in endemic pockets with a special focus on malaria and fluorosis.
Surakshit Matratva Ashwasan (SUMAN):
- The Surakshit Matritva Aashwasan (SUMAN) has been launched by the Ministry of Health and Family Welfare in 2019.
- It aims to provide assured, dignified and respectful delivery of quality healthcare services at no cost and zero tolerance for denial of services to any woman and newborn visiting a public health facility in order to end all preventable maternal and newborn deaths and morbidities and provide a positive birthing experience.
- Under the scheme, all pregnant women, newborns and mothers up to 6 months of delivery will be able to avail of several free health care services such as four antenatal check-ups and six home-based newborn care visits.
Anmol app:
- It is a multifaceted mobile tablet-based android application of the Ministry of Health & Family Welfare (MoHFW) for early identification and tracking of the individual beneficiary.
- The application would help to ensure tracking of beneficiaries for proper health care and promote family planning methods being adopted by them. The system also facilitates to ensure timely delivery of full competence of antenatal, postnatal & delivery services and tracking of children for complete immunization services.
LaQshya – Labour Room Quality Improvement Initiative
- This program focuses on Public Health facilities to help. They will be assisted by helping them improve their maternity operation theatres, and help augment the quality of care in labour rooms.
- This program will be implemented in all Community Health Centres (CHC), First Referral Unit (FRU), District Hospitals, Medical College Hospitals.
Pradhan Mantri Matru Vandana Yojana (PMMVY)
- Pradhan Mantri Matru Vandana Yojana (PMMVY) is implemented by the Ministry of Women and Child Development.
- PMMKVY came into effect from 1st January 2017.
- This Maternity Benefit Program is implemented in all districts.
- On fulfilling certain conditions, the beneficiaries would receive Rs 5,000 in 3 instalments.
- Cash benefits would be directly transferred to the bank accounts of the beneficiaries.
- Pradhan Mantri Matru Vandana Yojana – Common Application Software (PMMVY – CAS) is used for monitoring this program.
Janani Suraksha Yojana (JSY)
- This scheme is completely sponsored by the Government of India.
- Janani Suraksha Yojana comes under the National Health Mission.
Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA)
- This program was launched with the objective of detecting and treating cases of anaemia.
Population and Economic Development of India
Population and development are correlated. It is stated that the size of population, rate of growth and population composition, and its geographical distribution are important factors in determining the requirements of infrastructure, such as education, housing, health services, food supply, etc. Productive health capacity is also determined by the size and growth rate of population.
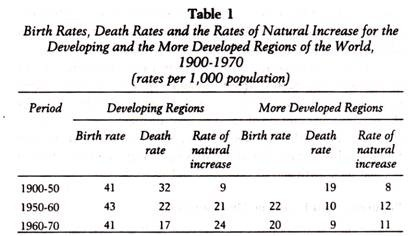
Thus, to make development plans for the present as well as for the future, there is a need to understand the structure and growth of population. A comparison of the developing countries and the more developed countries shows that the birth rate has been high in both categories, but the difference is still quite significant. Table 1 shows the facts in this context.
The developing countries are faced with several contradictions ‘n regard to population growth and economic and social development. For example, the birth rate has largely been static from 1900 to 1970, and the death rate has declined considerably because of the development in scientific and economic fields.
Thus, the increase in the population has been phenomenal – almost three times – from 1900 to 1970. The increase in the population of the developed countries has been just nominal. The birth rate has also declined to the extent of nearly 20 per cent. This clearly shows that along with scientific, technological and educational factors, population is a very important variable in economic development.
Since 1970 we notice a phenomenal change in birth and death rates and rate of natural increase in both developing and more developed countries. In 2002, in the developing countries, birth rate had declined to 24 from 41, and death rate to 8 from 17 per thousand.
Natural increase also declined from 24 to 16. The birth rate was also on decline in developing countries as from 20 it slide down to 11. Death rate was nearly stable as it was 9 in 1970 and 10 in 2002. However, natural increase declined to 1 from 10. Thus, the pressure of population is still a vital factor in the developing countries.
Several studies in developing countries have examined correlations between fertility levels in these countries and their social and economic development. These studies indicate that “improving economic and social conditions is not likely to have much impact in bringing down fertility in developing countries until a certain threshold level of development is achieved”. Since 1950s, the developing countries have shown their genuine concern for formulating suitable population policies.
Migration
Meaning of Migration:
Migration is the third factor for changes in the population, the other being birth rate and death rate. As compared to birth rate and death rate, migration affects the size of population differently. Migration is not a biological event like birth rate and death rate, but is influenced by the social, cultural, economic and political factors.
Migration is carried by the decision of a person or group of persons. The changes occurring in the birth rate and death rate do not affect the size and structure of the population on a large scale, while migration, at any time, may cause large scale changes in the size and structure of the population.
The study of migration is of vital importance because the birth rate, death rate and migration determine the size of population, the population growth rate and thus the structure of population. In addition, migration plays an important role in determining the distribution of population and supply of labour in the country.
Thus, the study of migration is also useful for formulating economic and other policies by the government, economists, sociologists, politicians, and planners along with demographers
Migration shows the trends of social changes. From the historical viewpoint during the process of industrialisation and economic development, people migrate from farms to industries, from villages to cities, from one city to another and from one country to another. In modern times, technological changes are taking place in Asia, Africa and Latin America due to which these regions are witnessing large-scale migration from rural to urban areas.
Economists are interested in the study of migration because migration affects the supply of skilled and semi-skilled labourers, development of industries and commerce causing changes in the employment structure of the migrated people. Formulation of economic policies has a close relation with the process of migration because migration affects the economic and social development of a country.
Out of the many side effects of the population growth in India and other developing countries, an important effect of industrialisation and economic development is the internal migration of the population on a large scale, which has drawn the attention of planners and formulaters of economic policies. Thus, migration is a demographic event, whose long term effects fall on the socioeconomic and cultural development of any region or country.
Migration is the movement of people between regions or countries. It is the process of changing one’s place of residence and permanently living in a region or country. According to the Demographic Dictionary of United Nations, “Migration is such an event in which people move from one geographical area to another geographical area. When people leaving their place of residence go to live permanently in another area then this is called migration.”
Migration may be permanent or temporary with the intention of returning to the place of origin in future.
Types of Migration:
Migration is of the following types:
(i) Immigration and Emigration:
When people from one country move permanently to another country, for example, if people from India move to America then for America, it is termed as Immigration, whereas for India it is termed as Emigration.
(ii) In-migration and Out-migration:
In-migration means migration occurring within an area only, while out-migration means migration out of the area. Both types of migration are called internal migration occurring within the country. Migration from Bihar to Bengal is in-migration for Bengal, while it is out- migration for Bihar.
(iii) Gross and Net Migration:
During any time period, the total number of persons coming in the country and the total number of people going out of the country for residing is called gross migration. The difference between the total number of persons coming to reside in a country and going out of the country for residing during any time period is termed as net migration.
(iv) Internal Migration and External Migration:
Internal migration means the movement of people in different states and regions within a country from one place to another. On the other hand, external or international migration refers to the movement of people from one country to another for permanent settlement.
Concepts Relating to Migration:
Besides, the following concepts are used in migration:
(i) Migration Stream:
Migration stream means the total number of people migrating from one region to another or from one country to another for residing during a time period. It is, in fact, related to the movement of people from a common area of origin to a common area of a destination. For example, migration of Indians to America during a time interval.
(ii) Migration Interval:
Migration may occur continuously over a period of time. But to measure it correctly, the data should be divided into intervals of one to five or more years. The division relating to a particular period is known as migration interval.
(iii) Place of Origin and Place of Destination:
The place which people leave is the place of origin and the person is called an out-migrant. On the other hand, the place of destination is the place where the person moves and the person is called an in-migrant.
(iv) Migrant:
Migrant is the labour which moves to some region or country for short periods of time, say several months or a few years. It is regarded as a secondary labour force.
Effects of Migration:
Internal migration affects the place where from people migrate and the place to which they migrate. When the migrants move from rural to urban areas, they have both positive and negative effects on the society and economy.
(i) Effects on Rural Areas:
Migration affects rural areas (the place of origin) in the following ways:
1. Economic Effects:
When population migrates from rural areas, it reduces the pressure of population on land, the per worker output and productivity on land increases and so does per capita income. Thus family income rises which encourages farmers to adopt better means of production thereby increasing farm produce.
Those who migrate to urban areas are mostly in the age group of 18-40 years. They live alone, work and earn and remit their savings to their homes at villages. Such remittances further increase rural incomes which are utilised to make improvements on farms which further raise their incomes. This particularly happens in the case of emigrants to foreign countries who remit large sums at home.
Moreover, when these migrants return to their villages occasionally, they try to raise the consumption and living standards by bringing new ideas and goods to their homes. Modern household gadgets and other products like TV, fridge, motor cycles, etc. have entered in the majority of rural areas of India where larger remittances flow from urban areas.
Further, with the migration of working age persons to urban areas the number of farm workers is reduced. This leads to employment of underemployed family members on the farm such as women, older persons and even juveniles.
Further, out-migration widens inequalities of income and wealth in rural area families which receive large remittances and their incomes rise. They make improvements on their farms which raise productivity and production. These further increase their incomes. Some even buy other farm lands. Thus such families become richer as compared to others, thereby widening inequalities.
2. Demographic Effects:
Migration reduces population growth in rural areas. Separation from wives for long periods and the use of contraceptives help control population growth. When very young males migrate to urban areas, they are so influenced by the urban life that they do not like to marry at an early age.
Their aim is to earn more, settle in any vocation or job and then marry. Living in urban areas makes the migrants health conscious. Consequently, they emphasise on the importance of health care, and cleanliness which reduces fertility and mortality rates.
3. Social Effects:
Migration also affects the social set-up of rural communities. It weakens the joint family system if the migrants settle permanently in urban areas. With intermingling of the migrants with people of different castes and regions in cities, they bring new values and attitudes which gradually change old values and customs of ruralites. Women play a greater role in the social setup of the rural life with men having migrated to towns.
(ii) Effects on Urban Areas:
Migration affects urban areas (or the place of destination) in the following ways:
1. Demographic Effects:
Migration increases the population of the working class in urban areas. But the majority of migrants are young men between the ages of 15 to 24 years who are unwed. Others above this age group come alone leaving their families at home.
This tendency keeps fertility at a lower level than in rural areas. Even those who settle permanently with their spouses favour small number of children due to high costs of rearing them. The other factor responsible for low fertility rate is the availability of better medical and family planning facilities in urban areas.
2. Economic Effects:
The effects of migration on income and employment in urban areas are varied depending upon the type of migrants. Usually the migrants are unskilled and find jobs of street hawkers, shoeshine boys, carpenters, masons, tailors, rickshaw pullers, cooks and other tradesmen, etc.
These are “informal sector” activities which are low paying. But, according to the ILO, the evidence suggests that the bulk of employment in the informal sector is economically efficient and profit-making. Thus such migrants earn enough to spend and remit to their homes.
Other migrants who are educated up to the secondary level find jobs as shophelpers, assistants, taxi drivers, repairing machines and consumer durables, marketing goods and in other informal activities that are small in scale, labour intensive and unregulated. Their earnings are sufficient to bring them in the category of a common urbanite with an income level higher than the unskilled workers.
Another class of migrants that is very small is of those who come for higher education in colleges and institutes to towns. They find good job in the “formal sector”, get good salaries, and follow a good standard of living. These are the persons who remit large sums to their homes and help in modernising the rural scenario.
(iii) Adverse Effects of Rural-Urban Migration:
Migration from rural to urban areas has a number of adverse effects. Towns and cities in which the migrants settle, face innumerable problems. There is the prolific growth of huge slums and shantytowns. These settlements and huge neighbourhoods have no access to municipal services such as clean and running water, public services, electricity, and sewage system.
There is acute housing shortage. The city transport system is unable the meet the demand of the growing population. There are air and noise pollutions, and increased crime and congestion. The costs of providing facilities are too high to be met, despite the best intentions of the local bodies.
Besides, there is massive underemployment and unemployment in towns and cities. Men and women are found selling bananas, groundnuts, balloons and other cheap products on pavements and in streets. Many work as shoeshines, parking helpers, porters, etc.
Thus, urban migration increases the growth rate of job seekers relative to its population growth, thereby raising urban supply of labour. On the demand side, there are no enough jobs available for the ruralities in the formal urban sector for the uneducated and unskilled rural migrants.
Consequently, this rapid increase in labour supply and the lack of demand for such labour lead to chronic and increasing urban unemployment and underemployment.
Patterns of Migration
Pattern 1. Inter-State Migration:
Inter-state migration is internal migration. When people from one state of a country move to another state in the same country for permanent settlement, it is called inter-state migration. The size of people migrating from one place to another is small in India.
In the Census of 1961, the registration of 68.6 per cent out of the total population was done at their birth place which shows that only 31.4 per cent people migrated. In the 1971 Census, this number decreased to 29.5 per cent.
Inter-state migration during 1961-71 shows that people from Uttar Pradesh, Kerala, West Bengal, Andhra Pradesh, Karnataka, Punjab, Rajasthan, Tamil Nadu, Nagaland, Gujarat, Jammu & Kashmir and Bihar respectively migrated. Migration was continuously occurring in Maharashtra, Delhi, Madhya Pradesh, Assam and Gujarat.
During 1951-61 migration occurred from Jammu & Kashmir and Rajasthan, Bihar and Tamil Nadu to other states, while during 1961- 71, migration from other states occurred into these states. Thus, during 1951-61, these states were population losing states. During 1961-71, these states came under the category of population gaining states.
The inter-state migration data reveal that the highest population (6.41 per cent) migrated from other states to West Bengal in 1961 which is an industrially developed state, while the least people migrated to Jammu & Kashmir, which is a backward state. Similarly, the highest population (6.49 per cent) migrated to other states from Punjab; while the least population (0.98 per cent) migrated to other states from Assam.
During 1971-81, there were no important changes in the trends of migration. There was no significant change even in the size of population coming in Maharashtra from other states through migration. The highest population (3.7 per cent) migrated to Maharashtra from the northern states (Bihar, Punjab, etc.).
The migration stream from 1981 to 1991 shows that population from Uttar Pradesh, Bihar, Rajasthan, Punjab and Andhra Pradesh migrated mainly to Maharashtra, Bengal, Assam and Karnataka. In the inter-state migration, the role of female has been of much importance.
This is because females after their marriage settle at the place of their husbands. The marriage and migration rate being the same in almost all the states, no serious problem arises. People largely migrate to Delhi and other metropolitan cities because opportunities of employment, educational and other facilities are available there.
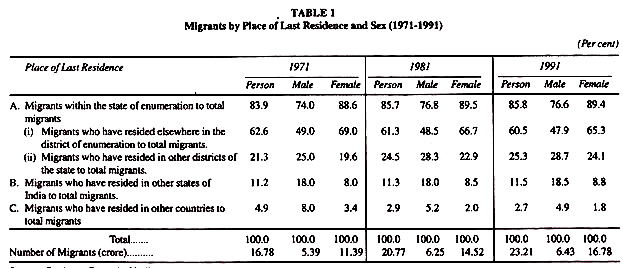
Pattern 2. Migrants by Place of Last Residence and Sex:
In India, the migrants by place of last residence and sex are shown in Table 1. The total number of migrants were 23.21 crores in 1991 which come to around 27 per cent of the Indian population. In sex-wise migration, the number of female migrants during 1971-91 due to socio-economic development in India, had increased by about 38 per cent.
The table reveals that most of the migration was short distance migration. This is because nearly 65 per cent of the migrants were enumerated in the same districts and nearly 90 per cent of the migrants were enumerated in the same state.
The table also shows the decrease in the international migration from 1971 to 1991. In 1971 the international migration accounted for 4.9 per cent of the total population while in 1991 it accounted for only 2.6 per cent of the total population.
The data for sex-wise migration by place of last residence indicates that females outnumbered males in the short distance migration, while males outnumbered females in the long distance migration.
Push Factor and Pull Factor of Migration
- Push factors:
- These factors force the people to move.
- These are negative factors associated with the current place or nation in which a person lives.
- Some of the push factors are worsening climate, unstable government and lack of job opportunities.
- Pull factors:
- These are certain positive factors associated with the new place, that people are moving into.
- Some of the pull factors are better standard of living, educational centres and better job opportunities.
Lees Theory of Migration
Everett Lee in his A Theory of Migration divides the factors that determine the decision to migrate and the process of migration into four categories:
1. Factors associated with the Area of Origin:
There are many factors which motivate people to leave their place of origin to outside area. They are push factors.
2. Factors associated with the Area of Destination:
There are very attractive forces at the area of destination to which the proportion of “selectivity” migrants is high. According to Lee, such forces are found in metropolitan areas of a country. Pull factors are present in such areas.
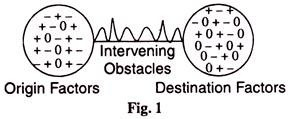
3. Intervening Obstacles:
There are intervening obstacles like distance and transportation which increase migrant selectivity of the area of destination. These obstacles have been lessened in modern times with technological advances. Lee also refers to cost of movements, ethnic barriers and personal factors as intervening obstacles.
4. Personal Factors:
Lastly, it is the personal factors on which the decision to migrate from the place of origin to the place of destination depends. In fact, it is an individual’s perception of the ‘pull and push forces’ which influence actual migration. He categorises these forces into “pluses” and “minuses” respectively. In other words, pluses are pull factors and minuses are push factors. In between them are “zeros” which balance the competing forces.
These are explained in Fig. 1, where the first circle represents the area of origin and the second circle the area of destination. The sign pluses represents the forces that attract people to a place (pull factors) and that of minuses represents the forces that push people from the area. Zeros represent the indifference of the people towards migration. In between these forces are the intervening obstacles.
According to Lee, it is the personal factors such as age, sex, race and education which alongwith the pull-push factors and intervening obstacles that determine migration. Further, there are sequential migrants such as children and wives of migrants who have little role in the decision to migrate.
Lee has formulated three hypotheses within the conceptual framework of the above noted four factors.
These are:
1. Characteristics of Migrants:
The following are the characteristics of migrants:
(1) Migration is selective.
(2) Migrants who respond primarily to plus factors at destination tend to be positively selective.
(3) Migrants who respond primarily to minus factors at origin tend to be negatively selective, or where they are overwhelming for the entire group, they may not be selective at all for migration.
(4) When all migrants are considered together selection for migration tends to be bimodel.
(5) The degree of positive selection increases with the difficulties of intervening obstacles.
(6) The characteristics of migrants tend to be intermediate between the characteristics of the population of the place of origin and those of place of destination.
(7) The higher propensity to migrate at certain stages of the life-cycle is important in the selection of migrants.
2. Volume of Migration:
The volume of migration is determined by the following factors:
(1) The volume of migration within a territory changes with the degree of areas included in it.
(2) It varies with the diversity of the people.
(3) It is related to the difficulty of evercoming the intervening variables.
(4) It varies with fluctuations in the economy.
(5) It varies with the state of progress in a country or area.
(6) Unless severe checks are imposed, both the volume and rate of migration tend to increase with time.
3. Streams and Counter-streams of Migration:
The following factors determine streams and counter-streams of migration:
(1) Migration tends to take place largely within well-defined streams.
(2) For every major migration stream, a counter-stream also develops.
(3) The efficiency of the stream and the counter- stream tends to be low if the place of origin and the place of destination are similar.
(4) The efficiency of the stream will be high if the major factors in the development of a migration stream are minus factors at origin.
(5) The efficiency of the stream will also be high if the intervening obstacles are great.
(6) The efficiency of a migration stream changes with economic conditions of the country, being high during prosperity and low during depression.
Lee concludes that migration is always selective and influenced by pull- push factors. Areas having plus factors are first selected for migration. It is generally the pull factors which lead to migration to urban areas rather than push factors, even though intervening obstacles do influence migration.
Harris – Todaro Model
“The Harris-Todaro model is useful in explaining internal migration but cannot explain international migration.” (a) Discuss the statement above, with a focus on the assumptions of the model. (b) Is the available empirical evidence consistent with the statement? Discuss. (c) Discuss the implications of migration restrictions and wage subsidies in achieving an efficient allocation of labour across sectors. Would reducing the inequality in land holdings promote efficiency in allocation?
The Harris-Todaro model was created to explain how internal migration occurs from rural to urban sectors through the difference in the expected wage. Pritchett points out that migration can benefit developing countries and their population much more significantly than any aid attempts. Industrial world transfer are around $70bn a year in aid, but by simply allowing a 3% rise in their labour force (taken up by migrants), the gains would be $300 billion: 4.5x greater. Fundamentally it was used to explain migration within an economy, but we attempt to expand the model to an international level. The model begins by accepting that the assumption of (near) full employment in urban labour markets isn’t particularly appropriate for developing countries which are beset by a chronic (under/)unemployment problem whereby many uneducated and unskilled rural migrants cannot find a job in the formal sector so become unemployed or join the informal sector. Thus in deciding whether to move to the city or stay at home on the farm, an individual has to weigh up the probability and risks of being unemployed for a considerable period of time against the positive urban-rural real income differential.
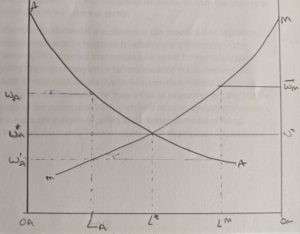
The graph above shows the AA line – the MPL of the rural sector – which is hence the demand for rural labour, whilst the MM line gives demand for manufacturing labour. The total labour force is of size OAOM. The efficiency wage Wm is paid in the manufacturing sector which is higher than the market clearing wage rate of w*. Due to the efficiency wage only LM workers are employed in the urban sector than the L* under a market clearing wage. If we assume that there is no-unemployment then OMLM workers would be employed in the urban sector whilst OALM would be employed in the rural sector at a wage of w’A. This would mean that a rural-urban wage gap would exist and some rural workers would wish to migrate. If we let LUS be the total urban labour pool then workers from the rural sector would migrate to the urban sector until the wage rate in agriculture equilibrated with the probability of finding a job in the manufacturing sector times the wage in the manufacturing sector:
wA = (LM/LUS)*wM
We would end up at a situation where now only LA workers are employed in the rural sector and LM are employed in the manufacturing sector, meaning that the difference (OMLA-OMLM) are unemployed workers. We should note that it wasn’t irrational for these workers to migrate: they rationally decided that it made sense – based on the rural-urban wage differential and the probability of them finding a job – to move. Unfortunately our model is constrained in assuming that these workers are completely unemployed, whereas in reality they may receive an informal sector wage and this would increase their expected income and thus means it makes more sense for rural migrants to migrate. Hence if we included this in our model we would see even greater “unemployment”, i.e. more migrants would move from the country to the city and end up in the informal sector.
Probably the most fundamental assumption in this model is that migration is an economic phenomenon in response to urban-rural differences in the expected income. This assumes that people only move for monetary gains, when in reality there are many other factors involved in this decision. For example, a lot of migration occurs due to humanitarian reasons as a result of conflict or disease – for example, the huge influx of migrants from the Middle East to Europe in the summer of 2015 is unlikely to be as a result of economic motives, but more for a desire of safety and a better standard of living. Therefore if we use the Harris-Todaro model to try and explain international migration (internal migration based on humanitarian/ethical grounds is perhaps unlikely, but not equal to zero: e.g. ethnic minorities may be more welcome in cities than rural areas and hence migrate) then we would be omitting a large chunk of migrants who move in order to escape persecution and death. Thus any further discussion on the use of the Harris-Todaro model implicitly assumes this factor, and acknowledges that a proportion of migration is outside the scope of our current model.
It may seem unrealistic for manufacturing firms to pay an efficiency wage, after all they can attract labour at the equilibrium rate. But this can be thought of as a wage necessary to ensure that workers have better nutrition (and so have higher productivity); reduce staff turnover; and ensure workers don’t shirk. If we try and explain the international migration process in a Harris-Todaro model we would say that rich countries (the “urban sector”) offer an efficiency wage which is higher than poor countries (the “rural sector”) in order to encourage them to migrate. So long as this expected wage difference is great enough (i.e. it includes the possibility that migrants will be unable to find jobs, as well as the costs of moving) then individuals from poor countries should move to rich countries in search for a job. In reality, the expected wage difference would be even greater than the market rate, due to the existence of unemployment benefits which means that developing country nationals would continue to migrate to the rich world, so long as unemployment insurance was sufficiently greater than rural wages and the cost of moving. This thus leads to political motives, in the developed world, to limit the amount of assistance given to migrant workers and perhaps curtail the amount of unemployment insurance they can receive.
The most fundamental criticism with this model is the barriers which exist preventing labour from migrating to rich (urban sector) countries from poor (rural sector). This makes it incredibly difficult to model international migration in a Harris-Todaro framework, simply because there are barriers to entry from workers wanting to move and not being able to do so. Furthermore, there are other barriers to entry, such as not speaking the language, cultural issues, not having a social or business network and needing sufficient capital to afford to physically move and then set up in a far away land.
Moreover, the model assumes that costs are given in a monetary sense, whereas in reality it might be quite difficult to put a value on leaving your family in a distant country to go and work abroad. Similarly, the model assumes that individuals can rationally calculate the economic gains from migration, but by moving individuals would be imposing a cost upon themselves, and would have to include the value of living abroad (i.e. even though wages are higher they are eaten up by housing, food, clothing and other living costs) which may be quite difficult to calculate.
Other issues with the model, in both an internal and international perspective, are that it doesn’t include human capital, there are no externalities and it treats workers and citizens as homogeneous. On the first issue, including human capital in the model is quite relevant, especially in an internationally empirical sense as developed countries allow more skilled workers than they do unskilled workers. Fundamentally this is because it is more politically feasible to do so, as skilled workers (e.g. doctors and electrical engineers) are often in short supply in the UK and the US and so are accepted by the public as a necessity. Also, skilled workers are (a) less numerous and (b) are less likely to compress the wages of the unskilled domestic residents in a developed country, and hence cause less concern that inequality will rise and that there will be problems associated with cultural assimilation and a burden on infrastructure. On the second issue, Carrington, Detragiache and Vishwanath, develop a model which incorporates a positive externality associated with earlier people moving from nearby villages and the probability of a rural citizen migrating. Because this increases the social network of a migrating individual it may increase the probability that he decides to move. This is anecdotally evidence in the UK through the clustering of nationals in certain parts of the country: in order to improve their social network and chance of acquiring employment. The third issue is a more interesting point, in that cities aren’t homogeneous: different cities develop different industrial sectors, and over time some of these sectors will boom whilst others will decline. This may mean that unemployment rates between cities vary and not only does a potential migrant have to decide whether he ought to move from agriculture to industry, but has to chose to which city he ought to move based on distance (and other costs), and returns (seeing which city is the most prosperous). This adds an even greater complex nature to such a model, especially with the large distances associated with cities in developed countries, and the different opportunities within them (e.g. Cardiff and New York). However, some would counter-argue that even the poorest cities in the developed countries, are much better off than the richest areas in developing countries.
To summarise, we see that the Harris-Todaro model is very limited in its scope in both an international and internal setting due to its narrow-mindedness assumption on economic values, which don’t incorporate emotional, social and humanitarian costs/benefits. More fundamentally, it isn’t an appropriate model in an international setting due to the barriers to entry which are erected by the developed world. By not incorporating human capital into our model, we are missing any migrants which may well be allowed into the developed world as high skilled workers can sometimes (but not always, even highly skilled workers can be limited to entering a country) get past the developed countries’ quota barriers. Todaro and Smith suggest that education for the sake of education should be restricted as a policy in developing countries, as often the urban sector can only ration jobs through education as a signalling effect. Whilst this seems like a bizarre idea, given that this would mean only the rich – who are generally the ones able to afford education in developing countries – would be able to attain jobs, and not poor, but clever productive individuals; it contradicts the policy prescription in an international setting, which ought to be for developing countries to increase their education so that workers become skilled and can improve their chances of migrating to developed country.
The movement of migrants from developing countries to developed countries, shouldn’t necessarily be seen as detrimental to the plight of developing countries, as proponents of “brain drain” theory suggest. Remittances sent by migrants to their families at home amount to $328bn, this can help developing countries provide education, health and give them a vital source of foreign exchange for the purchase of capital which can help them get out of poverty and low income traps.
Empirically we would expect most migrants to be of working age (i.e. between 18-50) and we would expect a lot more males to migrate than females, as there job – unfortunately – tend to be better. Whilst this may be the case overall, there is still substantial evidence that women, children and the elderly migrate, more than the economic model would suggest.
Furthermore, the fact that a significant proportion of migrants are not economic, but asylum seekers on humanitarian grounds would suggest that the Harris-Todaro model isn’t particularly useful in explaining world migration patterns.
Migration restrictions are imposed both in an international sense and sometimes internally – for example, see China, where nationals have to get permits (hukou) to reside in urban areas. The effect of this is to keep workers in rural areas to prevent a large source of unemployed workers in urban areas. The main reason for this is to prevent the social issues associated with overcrowding and the development of slums in urban areas. If deployed successfully – whilst being normatively unfair and ethically wrong – this could be quite successful at solving the issues associated with a swelling of urban populations and would maintain an equitable distribution of labour in rural areas. However this can be achieved, perhaps more effectively, and certainly more humanely, by increasing the benefits to staying in rural areas. For example by increase agricultural non-farm jobs. On the other hand wage subsidies are ineffective. A wage subsidy would increase the rural-urban expected wage differential (by either initially reducing unemployment, or through a higher urban wage) and thus encourage even more workers to migrate from farms to the city – in hope for a better life – creating even greater unemployment and would thereby fail in attempting to achieve an equitable labour distribution across sectors.
Reducing inequality in land holdings would only promote efficiency in allocation of workers between sectors if it increased the wages in rural areas. This may be unlikely if there are increasing returns to scale, but under the assumption of constant returns to scale it may be possible if we assume that tenants are more likely to invest in their own land (and hence increase returns and rural wages) than if they were working on somebody else’s land.
Urbanization
Introduction
- About:
- Urbanization refers to the population shift from rural to urban areas, the corresponding decrease in the proportion of people living in rural areas, and the ways in which societies adapt to this change.
- Causes of Urbanisation:
- Natural increase of population: It occurs when the number of births exceeds the number of deaths.
- Rural to urban migration: It is driven by pull factors (that attract people to urban areas) and push factors (that drive people away from the rural areas).
- Employment opportunities, educational institutions and urban lifestyle are the main pull factors.
- Poor living conditions, lack of educational and economic opportunities and poor health care facilities are the main push factors.
- Global Urbanisation:
- The most urbanized regions include Northern America (with 82% of its population living in urban areas (as of 2018)), Latin America and the Caribbean (81%), Europe (74%) and Oceania (68%).
- The level of urbanization in Asia is now approximately 50%.
- Africa remains mostly rural, with 43% of its population living in urban areas.
Urbanisation in India
- Urbanization Prospects:
- The World Urbanization Prospects, 2018 report produced by the UN Department of Economic and Social Affairs (UN DESA) notes that future increases in the size of the world’s urban population are expected to be highly concentrated in just a few countries.
- Together, India, China and Nigeria will account for 35% of the projected growth of the world’s urban population between 2018 and 2050.
- By 2050, it is projected that India will have added 416 million urban dwellers.
- Currently, India’s population stood at 1210 million in 2011, with an urbanisation level of 31.1% (Census of India 2011).
- State-wise Scenario:
- Number of Persons Living in Urban Areas:
- Over 75% of the urban population of the country is in 10 States: Maharashtra, Uttar Pradesh, Tamil Nadu, West Bengal, Andhra Pradesh, Gujarat, Karnataka, Madhya Pradesh, Rajasthan, and Kerala.
- Maharashtra leads with 50.8 million persons (13.5% of the total urban population of the country).
- Uttar Pradesh accounts for about 44.4 million, followed by Tamil Nadu at 34.9 million.
- Number of Persons Living in Urban Areas:
- High-Scoring States: Goa is the most urbanised State with 62.2% urban population.
- Tamil Nadu, Kerala, Maharashtra, and Gujarat have attained over 40% urbanisation.
- Among the North-Eastern States, Mizoram is the most urbanised with 51.5% urban population.
- Low-Scoring States: Bihar, Odisha, Assam, and Uttar Pradesh continue to be at a lower level of urbanisation than the national average.
- Union Territories: The NCT of Delhi and the UT of Chandigarh are most urbanized with 97.5% and 97.25% urban population respectively, followed by Daman and Diu and Lakshadweep (both above 75% urbanisation).
- India’s Global Commitments regarding Urban Development:
- The SDGs Goal 11 promotes urban planning as one of the recommended methods for achieving sustainable development.
- The UN-Habitat’s New Urban Agenda was adopted at Habitat III in 2016.
- It puts forth principles for the planning, construction, development, management, and improvement of urban areas.
- The UN-Habitat (2020) suggests that the spatial conditions of a city can enhance its power to generate social, economic and environmental value and well-being.
- Paris Agreement: India’s National Determined Contributions (NDCs) includes the goals to reduce the emission intensity of the country’s GDP by 33 to 35% by 2030 from 2005 level.
- India’s Initiatives for Urbanisation:
- Schemes/Programmes Related to Urban Development:
- Smart Cities
- AMRUT Mission
- Swachh Bharat Mission-Urban
- HRIDAY
- Pradhan Mantri Awas Yojana-Urban
- Government Initiatives for Slum Dwellers/Urban Poor:
- Pradhan Mantri Garib Kalyan Yojana
- Atmanirbhar Bharat Abhiyan (self-reliant India)
Significance of Urban Living
- Easier Access to Facilities: Urban living is linked with higher levels of literacy and education, better health, longer life expectancy, greater access to social services and enhanced opportunities for cultural and political participation.
- Urbanisation is associated with easier access to hospitals, clinics and health services in general.
- Living in proximity to these services results in improved emergency care and general health.
- Urbanisation is associated with easier access to hospitals, clinics and health services in general.
- Access to Information: There are also benefits from easier access to sources of information such as radio and television which may be used to communicate information about health to the general public.
- For instance, women living in towns and cities are more likely to be informed about family planning which results in reduction in family size and less frequent childbirth.
- Individualism: Multiplicity of opportunities, social diversity, lack of familial and social control over decision making leads to more self interest and facilitates decision-making by an individual and choosing one’s career and actions by oneself.
Issues Associated to Urbanisation
- Excessive Population Pressure: On the one hand, the rural-urban migration accelerates the pace of urbanisation, on the other, it creates excessive population pressure on the existing public utilities.
- Consequently, the cities suffer from the problems of slums, crime, unemployment, urban poverty, pollution, congestion, ill-health and several deviant social activities.
- Overflowing Slums: There are about 13.7 million slum households in the country sheltering a population of 65.49 million people across the country.
- As much as 65% of Indian cities have adjoining slums where people live in small houses adjacent to each other.
- Inadequate Housing: Among the numerous social problems of urbanisation, the problem of housing is the most distressing.
- A vast majority of urban population live under conditions of poor shelter and in highly congested spaces.
- In India, more than half of the urban households occupy a single room, with an average occupancy per room of 4.4 persons.
- Unplanned Development: The model of building a developed city comprises unplanned development, which only bolsters the dichotomy prevailing in urban cities between the rich and the poor.
- Pandemic-Induced Problems: The Covid-19 pandemic has exacerbated the misery of urban poor or slum dwellers.
- The sudden implementation of complete Covid lockdown severely affected the ability of slum dwellers to earn their living.
- Non-Inclusive Welfare Schemes: The benefits of welfare schemes for urban poor often reach only a small part of the intended beneficiaries.
- Most relief funds and benefits do not reach slum dwellers, mainly because these settlements are not officially recognised by the government.
Way Forward
- Sustainable Urbanization for Successful Development: As the world continues to urbanize, sustainable development depends increasingly on the successful management of urban growth, especially in low-income and lower-middle-income countries where the pace of urbanization is projected to be the fastest.
- Integrated policies to improve the lives of both urban and rural dwellers are needed, while strengthening the linkages between urban and rural areas, building on their existing economic, social and environmental ties.
- Improving Access to Health Facilities & Welfare Schemes: Accelerating efficiency of welfare and relief schemes along with ensuring access to free vaccines, food security and adequate shelter in the slums.
- Improving sanitation and transportation facilities in slums and establishing clinics and healthcare facilities.
- Aiding nonprofits and local support bodies who have better reach to these marginalised communities.
- New Approaches for Urbanisation: New approaches to urban planning and effective governance are the need of the hour.
- Necessary actions should be taken to build sustainable, robust and inclusive infrastructure.
- Instead of a top-down approach, a bottom-up approach shall be adopted to better understand unique challenges faced by the urban poor.

Industrialisation and Urbanisation in India
Industrialisation is the process of conversion of any given agrarian society into an industrial society. Industrialisation involves social and economic changes and extensive reorganisation of the economy for manufacturing. Earlier, the industries mainly depended upon the use of fossil fuels. However, with the development of new technologies, green revolution, and other sustainable practices, the use of fossil fuels has reduced to a great extent. As mentioned, urbanisation is the migration or shifting of rural populations towards urban areas. It can be for job opportunities or the better lifestyle that urban areas provide. Due to the greater rate of urbanisation, the number of towns and cities continuously increases. According to a study, 64% of developing countries and 86% of the developed countries will be urban. There are more chances of urbanisation in Africa and Asia (also in India). Industrialisation and Urbanisation in India are interlinked, as the increase in industrialisation increases job opportunities. These opportunities attract rural people, especially younger generations.
Industrialisation
In industrialisation, the cities establish multiple factories creating job opportunities that attract the rural population. The factories demand high labour and capital for the establishment and proper functioning. Industrialisation offers excellent economic opportunities for small and large-scale industries. Industrialisation provides better technological facilities for the progressive economy of the country. The first Prime Minister of India, i.e., Jawaharlal Nehru, started industrialisation to provide employment and decrease poverty in the country. This concept pushes the country forward towards self-sufficiency.
Let’s understand the various industrial policies and their objectives.
Objectives of Industrial Policy
- To achieve sustainable productivity growth
- Increase employment and eradicate poverty
- Better usage of available resources
- To compete with international organisations
- To make India a major partner globally
Policies of industrialisation in India
Industrial Policy Resolution of 1948– The industrial policy resolution of 1948 makes clear that India should have a Mixed Economic model. According to this policy, the industries are classified into four categories:
- Strategic Industries.
- Basic/Key Industries.
- Important Industries (Controlled Private Sector).
- Other Industries.
Industrial Policy Statement of 1956: The main objective of this policy was to revise the policy of 1948. This policy is often famous as the “Economic Constitution of India.” The main objectives of this policy included:
- Urgency of expanding the public sector.
- Need to grow the cooperative sector.
- Encouragement of the separation of ownership and management in industries.
- Prevention of the rise of private monopolies.
- Emphasis on cottage and small-scale industries.
According to the Industrial Policy Statement 1956, industries are classified into three categories, namely Section A, Section B, and Section C.
Drawback: It reduces the scope of expansion of private sector industries.
Industrial Policy Statement 1977: The postulates of the policy of 1977 are as follows:
- It aims to improve cottage and small industries.
- The policy classified the small-scale sector into three categories: cottage, small-scale, and small.
- In this policy, the government encourages workers’ participation in management from shop floor to broad level.
Drawback: It had the absence of measures in curbing the dominating position of large-scale units.
Industrial Policy of 1980: The main aims of this policy are as follows:
- This policy promotes economic federation.
- It raises the efficiency of the public sector industries.
- Reversing the previous three years of the trend of industrial production.
- Regain the faith in MRTP (Monopolies and Restrictive Trade Practices) Act.
- Reaffirmation of the belief in the FERA (Foreign Exchange Regulation Act).
New Industrial Policy (Economic Reforms of 1991): As launched by the Indian government in 1991, this new policy aims to provide economic stability in the country. It aims to raise efficiency. It also aims to de-reservation of public sectors.
Urbanisation in India
Several causes lead to urbanisation in India. These are as follows:
- Industrialisation: As already mentioned, industrialisation increases job opportunities. These opportunities attract rural people. There are lesser job opportunities other than agriculture in rural areas. The young generation is more attracted to exploring various urban job opportunities
- Better Lifestyle: There are many social causes such as better facilities, lifestyle, and great medical facilities of an urban area that attracts the rural population
- Better Technology: No doubt technology is the need of the hour. The urban areas are much better developed in technology than rural areas
The disadvantages of urbanisation in India
The disadvantages or impacts of urbanisation in India are as follows:
- Poor air quality
- Bad water quality
- Insufficient availability of resources
- High energy consumption
- Problems in waste disposal
Conclusion
Industrialisation and urbanisation in India are greatly interlinked. One of the main causes of urbanisation is industrialisation in India. Industrialisation provides excellent job opportunities to the citizens. The government of India took several measures and policies to improve industrialisation in India. Urbanisation is the migration or shifting of rural population towards urban areas that can cause disturbance in normal balance or ratio of urban-rural population. The disadvantages or impacts of urbanisation in India are Poor air quality, Bad water quality, insufficient availability of resources, high energy consumption, etc. The government is trying to develop the rural areas and increase employment there.
Population Policies
Population Policies formulated to address the unmet needs for contraception, health care infrastructure, and health personnel, and to provide integrated service delivery for basic reproductive and child health care. The main objective is to achieve a stable population at a level consistent with the requirements of sustainable economic growth, social development, and environmental protection.
Five-Year Plans by the Government of India for population control
First Five Year Plan: India is the first country in the world to begin a population control programme in 1952. It emphasized the use of natural devices for family planning.
Second Five Year Plan: Work was done in the direction of education and research and the clinical approach was encouraged.
Third Five Year Plan: In 1965, the sterilization technique for both men and women was adopted under this plan. The technique of copper- T was also adopted. An independent department called the Family Planning Department was set up.
Fourth Five-Year Plan: All kinds of birth control methods (conventional and modern) were encouraged.
Fifth Five Year Plan: Under this plan the National Population Policy was announced on 16 April, 1976. In this policy, the minimum age for marriage determined by the Sharda Act, 1929 was increased. It increased the age for boys from 18 to 21 years and for girls from 14 to 18 years. The number of MPs and MLAs was fixed till the year 2001 on the basis of the census 1971. Under this Plan, forced sterilization was permitted which was later on given up. In 1977, the Janata Party government changed the name of Family Planning Department to Family Welfare Department.
In the Sixth, Seventh and Eighth Plans, efforts were done to control population by determining long-term demographic aims.
Ninth Five-Year Plan: In 1993, the government had established an expert group under the chairmanship of M.S. Swaminathan for formulating national population policy. Though this group had prepared the draft of the new population policy in 1994, it was reviewed in 1999 by the Family Welfare Department and was passed by the Parliament in 2000. The Central Government formulated the ‘new national population policy’ in February 2000. This policy has three main objectives:
Objectives of Ninth Five Year Plan
1. Temporary objective: The easy supply of birth control devices was included in it. Besides, the development of health protection framework and recruitment of health workers were also made a part of it.
2. Middle-term objective: Under it, the total fertility rate (TFR) had to bring down to the replacement level of 2.1 by 2010.
3. Long-term objective: Under it, the Objective of population stabilization by 2045 is to be achieved.
The population has to be stabilised at that level which must be harmonious from the points of view of economic and social development and environmental protection.
It has been announced in the new population policy to keep the composition of the Lok Sabha unchanged by 2026 so that the states could co-operate without any fear. Under current provisions, the number of MPs in different states by 2001 has been determined on the basis of the census 1971. It was to be changed in 2001 on the basis of the new census report (2001). But it might be harmful to those states which had taken part in the population control programme with great fervour. Those states which had not laid proper attention on population control could get more shares in the Lok Sabha resulting in wrong effect on the population control programme. So, the Lok Sabha would not have more than 553 elected seats till 2026 and the number of Lok Sabha seats of each state would remain the same as it is at present. While announcing this new policy, the Central Health Minister said that the people living below poverty line would be rewarded properly if they would marry after 21 years, adopt the standard of two children and undergo sterilisation after two children.
The following major Objectives had been set in the National Population Policy till the year 2010:
1. The ‘total fertility rate’ to be reduced to 2.1.
2. The high class birth control services had to be made available publically so that the standard of two children could be adopted.
3. The infant mortality rate had to be reduced to 30 per thousand.
4. The mother mortality rate had also to be reduced to below 100 per one lakh.
5. The late marriage of girls had to be encouraged.
A high level 100-membered National Population Commission has been set up under the chairmanship of the Prime Minister on 11 May 2000 to supervise and analyse the implementation of this new population policy.
Evolution of Population Policy in India
According to United Nations projections, India is about to surpass China as the most populous country by 2027, adding approximately 230 million by 2050, the majority of whom will be amongst the world’s poorest. Ironically, India was one of the first countries to adopt a population control policy as early as 1952. Even so, the country’s population has risen significantly in the past 6 decades. To understand the path the policy has taken over the decades, its effects, and progressions, let us break down the policies into segments for easier understanding and retention.
Why Should We Understand Population Control?
India with only 2.4 percent of the world’s surface area had 16.7 percent of the world’s population as in 2001. The inclusion of policies has resulted in a decline in the death rate below 8 per thousand; on the other hand, the birth rate continues to be around 18 per thousand. The frightening rise in population aggravates problems like poverty, unemployment, inequalities, basic health, social security, etc. Population outweighs the existing resources which strain the pool available for the society to rely on, adding pressure on the environment and other natural resources to an extent of depletion and exploitation.
With an understanding of such potential problems due to high demand (larger population with limited resources), India had adopted a population policy. Let us understand its course over the decades step by step and what have been the impacts of the same.
Indian Population Policy Over The Decades
The primary objective of population control is to facilitate sustainable economic growth, social development, and environmental protection. Indian population control policies have seen several changes over different Five – Year plans by the Government of India.
First Five-Year Plan (1951-56)
In a report by India’s lead urban demographer, R.A Gopalswami, it was estimated that India’s population would grow by 5,00,000 every year, which caught the attention of the Indian Government, and the National family planning program was launched (the first country to undertake such a policy). Some of the key strategies were:
- Encouraging households to have only two children and spacing the birth of these children over two years.
- Rural areas were the primary target and a door-to-door campaign was initiated.
- Motivating families to adopt these families by monetary incentives.
- Spreading awareness of family planning via radio, television and newspaper.
Second Five-Year Plan (1956-61)
The idea was strengthened that high population growth would affect economic advancements and living standards per capita. The imbalance of availability of land and capital to population further deepened the idea that population growth has to be curbed to alleviate incomes and levels of living.
Along with the natural (Gandhian) approach, the clinical approach gained momentum in 1956. The report by Gopalswami suggested that mass sterilization was the best approach as it required a minor surgery without prolonged hospital visits. Some key strategies were:
- Voluntary sterilization facilities were created
- Contraceptive distribution was facilitated through primary health centres.
- They were either provided free or prices were reduced for low-income families.
The 1961 census indicated that both approaches turned out to be ineffective since people did not find it necessary, men had misconceptions about losing sexual drive, losing weight, and death.
Third Five-Year Plan (1961-66)
After 1962, the Indian Population control policy became an aggressive and imperative approach, as a high birth rate was perceived as the greatest obstacle to economic development. Some key strategies were:
- A separate department of Family planning was set up to set a goal of reducing the birth rate to 2.5% by 1972.
- State and district wise family planning goals were set.
- Increased the number of clinics five fold.
- As opposed to earlier approaches, a more extensive approach was adopted, to educate and impart knowledge by appointing a large number of educators.
Fourth Five-Year Plan (1969-74)
The purview of population control extended from economic development to that of social change. The importance of population control was recognized as unavoidable as equality and dignity of a man lies on both factors- economic growth and low rate of population growth.
- A new target was set to reduce the birth rate to 3.9% by 1974.
- A cafeteria approach was devised – all methods of contraception were made available.
- It included condoms, diaphragms, jelly, creams, foam tablets; the use of the intrauterine contraceptive device (IUCD) for couples with one or two children; sterilization for couples who do not want more children.
Sterilization became one of the main strategies for family planning.
- Medical Termination of Pregnancy Act was adopted to allow abortion performed by a medical practitioner with some exceptions.
- IUCD acceptance declined as bleeding and rumours spread.
- Mass vasectomy camps were organized and incentives were introduced to boost sterilization. The total number of acceptors reached 5.9 million by 1972-1973.
Fifth Five-Year Plan (1974-79)
Policymakers strongly believed that family size largely impacted general development strategy, as a result, a new target was set to reduce the birth rate from 3 % to 2.5 % by 1984.
Key strategies involved were:
- The minimum age of marriage was raised from 15-18 years for females and 18-21 years for males.
- Enacted compulsory sterilization and specific incentives and disincentives to family planning.
- Education about population problems became a part of the school curriculum.
- Female health workers were given financial incentives to meet yearly quotas.
Sixth Five-Year Plan (1980-85)
The government changed the name of the program from family planning into family welfare after the stringent and coercive policies aided to vote Gandhi out of power post Emergency.
- Maternal and child health services and nutrition became a part of the population control strategy.
- After the political fallout, more emphasis was put on providing incentives to attract people to understand and accept family planning.
- Long-term policies were set, as a result, targets were reduced.
Seventh Five-Year Plan (1985-90)
- The policy was divided into long and short term goals. Former being to fix the net reproduction rate and latter focused on female age at marriage and the practice of contraception.
- The focus was set on increasing the literacy rate, especially of women and increasing their employment opportunities.
- Implemented All-India Hospitals postpartum Program at district and sub-district level hospitals.
- Reorganized primary health care facilities in urban slum areas.
- Reservation of a specified number of hospital beds for tubal ligation operations.
- Remodelling of IUCD rooms in rural family welfare centres.
Despite such remarkable initiatives, the 1991 census showed that India still had one of the most rapid population growths globally.
Eighth Five-Year Plan (1992-97)
In 1996, the Government of India introduced a new population policy that focused on areas like employment, education, public health, human development as indirect measures to curb population growth.
- Shifted emphasis from couple protection rate to birth lowering rate.
- Involved non-government organizations and voluntary agencies in programs.
- Improving the status of women through training and infrastructure.
- Reducing the default preference of a male child of a family with one or two daughters by providing social security measures.
- Central government employees were given incentives for accepting the two children norm.
Ninth Five-Year Plan (1997-2002)
The National Commission on Population introduced a new plan called National Population Policy 2000 (NPP 2000). This new policy focused on areas like contraception, reproductive health care and health care infrastructure.
- Increased emphasis on spacing methods like IUCD.
- Fixed day static services at all facilities available.
- Established quality assurance committees to provide quality care in family planning services.
- Providing insurance for deaths, complications and failures caused by sterilization.
Tenth Five-Year Plan (2002-07)
There were several shifts from the ninth to the tenth plan:
- Demographic goals to focus on enabling couples to achieve their reproductive goals.
- Method specific targets to fulfil all unmet needs for contraception to reduce unplanned pregnancies.
- Women centred program to the health care needs of the family with involvement of men in Planned Parenthood.
- Supply driven service delivery to the need and demand-driven service and providing service provisions as per the convenience of the couple.
- Implementation of a program for health care for women and children, to reduce infant mortality and reduce high desired fertility.
Eleventh Five-Year Plan (2007-11)
The government extended more services, including delivery of contraceptives at the doorsteps, providing counseling for newly married couples, and compensation for sterilization. Since the shift in the approaches from quota-oriented to voluntary measures, India witnessed the effective implementation of strategies.
- Advocated fertility regulation through voluntary and informed consent.
- Addressed special health care needs of the elderly, especially those who are socially and economically vulnerable.
- Reduce infant mortality rate to 28 and maternal mortality rate 0 to 1 per 1000 births.
- Provide clean drinking water for all by 2009.
- Reduce anaemia among women and girls by 50% by the end of the plan.
- Ensure that at least 33% of the direct and indirect beneficiaries of all government schemes are women and girl children.
An overview of the Indian population control policy.
| 1952-61 | Service providing period | Focused on providing information and services to potential consumers, goals were not defined, less demand for services supplied by healthcare institutions. |
| 1962-1977 | Target-oriented period | Specific targets introduced, coercive measures taken to reach targets, shift from promotion of contraception to sterilization, coercive measures backfired and changed the political arena along with affecting the effectiveness of the policy. |
| 1977 | Voluntary/Target free policy | Adopted indirect population control measures such as health care, social development, and family planning services. More suitable and flexible for the Indian demographic. |
| 1980-2010 | 10-year population increase rate decreased from 25.9% between 1970-80 to 16.8% between 2000-2010 |
The reduction of the population could also be attributed to the accelerated socio-economic development since 1991. However, the Indian population control policies are not effective in comparison to the other countries in the world. India’s percentage of the world’s total population increased from about 15.7% in 1980 to about 17.8% in 2010, which means that the population growth rate in India was greater than the average growth rate in the world. India’s population may overtake China and become the most populous country in the world.
The lack of effectiveness of the policies can be attributed to the below:
- Policies are not well defined and change constantly.
- Implementation measures of strategies lack focus and shift periodically.
- Targets are not achieved and have to be revised frequently.
- A variety of reasons contribute to such inadequacies. Diversity is one of them.
- Other factors – 66% of the population lives in rural areas, 40% of women are illiterate, gender bias, the caste system still prevails, communal tension exists.
- Due to the interplay of such multifaceted factors, population control can be promoted not forced or implemented effectively.
- Poverty is another reason, as population spike has occurred mostly among the poorest population or poorer states. Comprehensive socio-economic development is required to tackle this aspect.
- When socio-economic conditions improve, the birth rate will be lower and overpopulation would significantly decrease.
Evolution of Family Welfare Programmes in India
The International conference on Population and Development held in 1994 established an international consensus on a new approach to policies to achieve population stabilization. In 1951 India became the first country in the world to launch a family planning programme to reduce population growth in the country.
The department of Family welfare undertook many pilot activities for implementation of the family welfare program to meet the needs of women who are at risk of unwanted births and has assisted the country to accelerate fertility decline. In 1997, India changed the strategy of National Family welfare program to Reproductive and child Health- and in the ninth five-year plan (1997-2002), a total change in implementation was recommended.
Reproductive health is the term, which covers all aspects of women’s health from child hood to adolescence, through reproductive age, menopause and beyond it. It is the integration of maternal health, child health and adolescent health into primary health, through which we hope to transform the population problem to population solution.
WHO defines reproductive health within the framework of definition of health as “A state of complete physical, mental and social wellbeing and not merely the absence of disease or infirmity, the reproductive health addresses, the reproductive processes,-functions and system at all stages of life.”
Reproductive health therefore implies that- People are able to have a responsible satisfying and safe sex life and that-they have the capability to reproduce and the freedom to decide, if when and how often to do so. This definition puts emphasis on right of men and women to be informed of and to have access to safe, effective, affordable and acceptable methods of fertility regulation of their choice and the right of access to appropriate health care services that will enable women to go safely through pregnancy and child birth- and provide couples, with-the best chance of having a healthy infant”.
Women’s health is important during all phases of their life. When she gives birth. She passes on the gift of good health to the next generation. A healthy child grows up into a healthy adolescent, good health during adolescent period leads to good health during reproductive years, the cycle Continues into the next generation when a healthy pregnant is able to give birth to a healthy child. RCH Program will go a long way towards improving the overall health of women and that of society as a whole.
In order to achieve reproductive health women empowerment is essential. It is also necessary that required changes be made in the social factors that hinder women overall development and their rights. Reproductive rights means women’s right to decide whether, when and how to have children – regardless of nationality, class, ethnicity, race, age, religion, disability, sexuality or marital status in the social, economical and political conditions that make such decisions possible.”
Family Welfare Programmes Mainly include:
1. Family planning information, counselling and services to women for healthy reproduction.
2. Education about safe delivery and post delivery of the mother and the baby and the treatment of women before pregnancy.
3. Health care for infants immunization against preventable diseases.
4. Prevention and treatment of sexually and Reproductive Tract infection.
A large number of people suffer from in-silence due to reproductive tract infection and sexually transmitted disease. RTI can cause pregnancy – related complications infertility and chronic pain. They are inflammatory disease and HIV. So an important object of the welfare program is the identification and tract infection.
Nearly 4 out of 10 currently married women in India report at least one reproductive health problem that – could be symptomatic of a more serious reproductive tract infection. The percentage of correctly married women with any reproductive health problem varies from 19 percent in Karnataka to 67 percent in Meghalaya.
Among women who report any reproductive health problem two-thirds have not seen any one for advice or treatment. Less than one third of women who seek advice or treatment for reproductive health problems go to government health professionals. So education regarding reproductive health, safe habits and syndrome treatment are the answer to create healthy mother who in turn will produce a healthy baby.
Keeping in view the issues and problems confronting reproductive and child health, various family welfare programmes have been effectively implemented in every state with a larger prospective intended for population stabilization, reduction of infant and Maternal mortality through integrated Family Welfare services, I.E.C act activities. (Information, Education and Communication activities) Immunization and prophylaxis against Anemia and Vitamin A deficiency of children and mothers with a comprehensive health strategy. It is a people centred programme. Government and community should support this programme.
The basic objective of the Family welfare programme is to stabilize the population and to provide qualitative health services including immunization to both-pregnant mother and children. Since the last 48 years, the Family welfare programme is being implemented in the State with financial assistance of the central Govt.
The family planning programme is not merely intended for population stabilization now but it has much larger perspective in holistic approach towards Reproductive and child health. Services, family planning, Immunization, training etc. comprise a comprehensive health care package. The Family welfare activities are guided as per the policies, guidelines and funding by Govt. of India.
To ensure qualitative healthy delivery and population control the Reproductive and child Health programme has been implemented in every state with community needs assessment approach. To boost the health care delivery, each State Govt. has formulated health reforms and implemented the same to give better autonomy to the health institutions.
Family Planning in India
For the success of family planning programme, there is need to motivate the people. India lives in villages where people are illiterate, ignorant and tradition bound. They think and act according to the rural value system. Even in urban areas, vast sections of the population hold on to old beliefs, traditions and values. The traditional joint family system is a barrier to the small family norm.
Family planning emphasises the fact that birth control is a scientific method by which a couple can control the size of family. The birth of a child is not the matter of fate but a matter under human control.
In many countries including India, the problem of population explosion is a major one. As a result of the efforts made by the Government for solving this problem, the concepts like family welfare and family planning have gained popularity. Family welfare puts stress on health, child care, protection against child diseases, caring of pregnant women, nutritious food, education, etc. along with birth control.
The programmes of family planning try to control the birth rate by changing the attitude of people towards the adoption of family planning techniques. Thus, family welfare and family planning lay emphasis on increasing the quality of the population which is possible only through population control.
Meaning of Family Planning:
Family Planning means Planned Parenthood. According to Robert McNamara, a former President of the World Bank, “Family planning is not designed to destroy families; on the contrary it is designed to save them.” The National Family Planning Programme, 1952 of India defines it as “reducing birth rate to the extent necessary to stabilise the population at a level consistent with the requirement of the National Economy.”
According to Dr. Rodhinorton, “Family planning means activities of determining the time period between the birth of children and the number of required children for the couple themselves along with the health and family welfare”. Thus, family planning is not just a method for population control but in a broad sense, it is concerned with the very quality of human life.
Family planning is a social movement which lays emphasis on the overall development of the family. As the basic aim of family planning is to limit the size of the family, married couples are convinced to adopt birth control methods and to have children by choice and not by chance. They are asked to follow small family norm and the slogan “Small Family, Happy Family.”
In India, family planning has been converted into family welfare programme which aims at providing material and child health care and contraceptive services. We should not forget what the 1951 Census Report stated, “If we are not allowing ourselves to die naturally, we should not allow birth naturally.”
Need for Family Planning in India:
India is the second most populous country in the world after China and is the home of 1/6th of the world population. But it has not more than 2.5 per cent of the global land. It is a resource-poor country with high population density of 324 per sq. km. High growth rate of population puts pressure on scarce resources resulting in reduction in per capita income, thereby retarding the development process.
Further, high population growth rate tends to retard social and economic development because it alters the age structure of the population, places a very heavy burden on education, employment, health services, food and natural resources and prevents the raising of the quality of life of Indians. Thus family planning is essential for an all round and sustained growth of the Indian Economy.
Family planning is beneficial not only for an individual but also for the Indian economy as a whole. Family planning leads to a reduction in birth rate of children and therefore the number of dependents in a family. As a result, children will be better looked after, fed and educated.
With less number of children to support, the standard of living of the family will improve. Thus family planning is necessary for better health and long life of mother and child and for overall prosperity and happiness of the family. When the standard of living of majority of families rises through family planning, the quality of life of the entire society improves.
Family planning is also necessary for rapid economic development of India. As the growth of population is reduced in absolute numbers, the per capita income will rise. Simultaneously, the growth rate of labour force will come down. This will have effect of improving the employment situation in the country and the unemployment problem will be solved to a considerable extent.
On the other hand, small families with less and healthy children, having better education and health services through family welfare programme bring out a healthy labour force. This will, in turn, raise productivity and income levels in the country. High incomes will raise the rates of saving, investment and capital formation and ultimately the growth rate of the Indian economy.
Thus family planning is needed not only to raise the quality of life of the Indian people but also the level of India’s economic development. On the other hand, economic growth improves employment opportunities and raises incomes, and family welfare improves the quality of life.
Thus, in brief, the need for family planning in India arises:
1. For rapid and sustained economic development of the economy;
2. For raising the living standards of the people;
3. For attaining and maintaining the optimum size of the population in keeping with our resources;
4. For improving the quality of population;
5. For maintaining the health of the mother and child; and
6. For making the population aware of available facilities relating to reproductive and child care programme and of small family norm.
Family Planning: Strategies and Outcomes:
Over the years, India has gone through a variety of family planning strategies of neutrality, experimentation, population control, maternal and child health care, etc. We discuss these strategies along with their outcomes (or results).
1947-1951:
The period following independence and before the beginning of the planning era was one of neutrality. During this period, health care services were primarily in the hands of private general practitioners who provided comprehensive, integrated and good quality services. But technology for detection of diseases and management of health problems was limited.
Health care services were mainly based in urban areas, were costly and so out of reach of the poor. Government hospitals and dispensaries were very few and in urban areas. Thus, the majority of population belonging to the poorer sections and those residing in rural areas did not have any health care facilities. As a result, death rates among women and children were quite high due to maternal morbidity and mortality.
1951-61:
During 1951-61, family planning as a method of population control, was started as the government programme. The Government of India launched the National Family Planning Programme in 1952 with the objective of “reducing birth rate to the extent necessary to stabilise the population at a level consistent with the requirement of the national economy.”
It was based on Clinical Approach to provide health care services in family planning centres set up by the Government in urban areas. Couples were motivated to visit such centres for maternal and child health care and family planning services. These centres persuaded couples to use contraceptives and undergo sterilization of one partner in case their family was complete.
Efforts were also made to extend family planning services to rural areas in some states under the block development programme. But there was slow progress due to resources and manpower constraints.
This was the period of experimentation in which these measures had no impact on the fertility rate, mortality rate and the natural growth rate of population because of poor outreach of family planning services in the country as a whole. The decadal growth rate of population was 21.5 per cent during this period.
1961-70:
During this period, the Extension Approach to family planning was adopted. This approach emphasied the adoption of an Educational Approach to family planning through Panchayat Samitis, Village Development Committees and other groups so as to change the attitudes, behaviour and knowledge of the people towards family planning in rural areas.
This was supplemented by the Camp Approach to provide care to children and pregnant women in order to improve access to immunization. Efforts were also made to provide the birth spacing method to rural women through camps.
The family planning programme was also target oriented and the target was to reduce the birth rate to 25 per 1000 persons by 1973. To make this programme more popular, Cafeteria Approach was adopted. Under it, the couples were given advice on different types of family planning methods to be adopted.
The choice of a particular method was left to them. For the effective working of the family planning programme, a separate department of Family Welfare was created in the Ministry of Health and Family Planning in 1966. Despite these approaches, the Department was unable to achieve any improvement in child and maternal health services due to the lack of infrastructure and manpower and follow-up services.
1970-79:
This period was the beginning of population control policy in which many new initiatives were undertaken during the Fourth Plan. They were:
(a) Social acceptability for a small family;
(b) Increasing information and knowledge about family planning methods both in urban and rural areas; and
(c) Making available various devices and equipment to the couples.
To make this programme more effective, Selective Approach was adopted under which couples in the reproductive age-group of 25 to 35 years were persuaded to undergo sterilisation. The Medical Termination of Pregnancy (MTP) Act, 1972 was passed which enabled women with unwanted pregnancy to obtain safe abortion services.
Another important measure was the integration of family planning services with improving the health and nutritional status of women and children. To tackle micro-nutrient deficiencies and under-nutrition among women and children, food supplements to pregnant and lactating women, and to preschool children were provided through primary health care and integrated child development services.
To control rapidly growing population, the National Family Planning Programme was included in the Fifth Plan. To implement it, monetary incentive was given to couples undergoing voluntary sterilisation. This was followed by massive compulsory sterilisation drive of 1976 during the Emergency which led to the sterilisation of 82.6 lakh people.
In the post-Emergency period, the family planning programme included:
(i) Fixing the marriage age for girls at 18 years and for boys at 21 years;
(ii) Making sterilisation voluntary;
(iii) Monetary incentive to those who go for sterilisation and tubectomy; and
(iv) Use of media for spreading family planning in rural areas, etc.
The Family Planning Programme was renamed as Family Welfare Programme and efforts were made to increase integration of family planning services with those of child and maternal health and nutrition services. The emphasis on voluntary sterilisation slowed down the Family Planning Programme. As a result, the number of sterilisations fell from 82.6 lakh in 1976-77 to 9 lakh in 1977-78.
1980-91:
The main strategy during this period was to intensify family planning and Maternity and Child Health (MCH) programmes. The National Health Policy was formulated in 1983 to provide comprehensive framework for planning, implementation and monitoring of MCH services.
A network of centres in urban and rural areas was established to provide these services. The Universal Immunization Programme (UIP) was started in 1986 which was extended to cover all districts by the end of 1990.
1992-2002:
To give a new thrust and dynamism to the family welfare programme, the Child Survival and Safe Motherhood Programme and the Social Safety Net Programme were started during the Eighth Plan to improve access to MCH services. To make these services successful, Community Needs Assessment Approach and Family Planning and Implementing programmes were started.
In October 1997, the Reproductive and Child Health (RCH) programme was started to stabilise population and improve quality of life by reducing maternal and infant mortality and morbidity, and assuring reproductive health and choice to couples.
It combines Fertility Regulation, Safe Motherhood, Child Survival, Universal Immunisation Programme (UIP), Reproductive Tract Infections (RTI), etc. These services are provided through secondary and tertiary health care centres in the country.
Since April 2001 under the National Maternity Benefit Scheme (NMBS) financial benefit of Rs. 500 per pregnancy is provided for first two live births to women who belong to households below poverty line and have attained 19 years of age or above.
Results:
The results (or outcomes) of the various family planning strategies over more than five decades are depicted in Table 33.1. The crude birth rate declined from 40.8 in 1951 to 25 in 2001 and total fertility rate per women also declined from 6.0 to 2.8 due to the various measures adopted to control births.
With improvement in maternal and child health care and nutritional status of the population, better medical facilities and control over killer diseases, the death rate and infant mortality rate have been considerably reduced. While the crude death rate declined from 25.1 in 1951 to 8 in 2001, and the infant mortality rate also declined from 146 to 64. Similarly, the child mortality rate declined from 57.3 in 1972 to 19.5 in 2001.
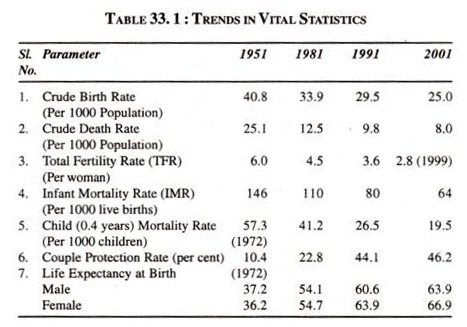
The Maternity and Child Health Care and Family Planning Programmes adopted over the years have not only increased the couple protection rate but also life expectancy at birth for both male and female population. The couple protection rate increased from 10.4 per cent in 1972 to 46.2 per cent in 2001. The life expectation at birth for male rose from 37.2 to 63.9 and for female from 36.2 to 66.9 over the period.
These results also reveal that India is following the demographic transition pattern of the third stage, where the death rate is declining faster than the birth rate due to better medical facilities and family, maternity and child welfare programmes of the government.
Achievements of Family Planning or Family Welfare Programme:
The Planning Commission and the Department of Family Welfare have been laying down targets for family planning, health and welfare activities in each Plan. Over the years, there have been progressive achievements in their targets.
Some of the major achievements in family welfare programme are:
1. 250 million births averted from 0.4 in 1971 to 250 in 2000.
2. Acceptors of family planning methods reached 59.4 million in 2000.
3. Reduction in crude birth rate from 40.8 in 1951 to 25.0 in 2001.
4. Reduction in crude death rate from 25.1 in 1951 to 8.0 in 1998.
5. Decline in total fertility rate from 6 in 1951 to 2.85 in 1998.
6. Reduction in infant mortality rate from 146 in 1951 to 64 in 2001.
7. Increase in couple protection rate from 10.4 per cent in 1971 to 46.2 per cent in 2001.
8. Increase in the expectation of life from 37 in 1951 to 63.3 in 2001.
9. The average annual growth rate of population declined from 2.22 per cent in 1971 to 2.14 per cent in 1991 and further to 1.93 per cent in the 2001 Census.
Thus technological advances in family planning methods, improvement in quality and coverage of health care, implementation of disease control programmes and increasing literacy and awareness have led to increased utilization of available health services. As a result, the family welfare programme has been quite successful.
Criticisms Against the Family Planning or Welfare Programme in India
Criticisms Against the Family Planning or Welfare Programme in India are as follows:
1. Multiple Approaches:
The Government has been experimenting with a variety of approaches to provide family planning services to the people. It started with a clinical approach, switched over to the extension approach, to target-oriented approach, to selective approach, to method specific targets approach, and to decentralised area specific planning approach since 1996. Such policy changes have created confusion and indecisiveness in the minds of the field staff connected with the family welfare programme.
2. Untrained Health Workers:
According to Pravin Vasaria, the health workers recruited by the Family Welfare Department are grossly ill-equipped for the difficult task assigned to them. They do not have proper training for primary health care and in particular maternal and child care for rural areas. Moreover, there is no system of feedback and interaction between health workers and their superiors stationed at the headquarters.
3. State Sponsored:
The family welfare programme in India is formulated, sponsored and financed by the Central Government uniformly throughout the country. But it is implemented by the States at their district, block and village level bureaucrats.
Such an indiscriminate and macro programme is counterproductive in India where there are diversities of castes, creeds, religions, customs, etc. Thus it is not keeping with local needs and circumstances of different types of people and is counter-productive.
4. Emphasis on Quantitative Targets:
As a corollary to the above, one of the main weaknesses of this state-sponsored programme has been to achieve quantitative method-specific targets of acceptors of family planning.
5. Inter-state Disparities:
The family welfare programme has failed to check inter-state disparities in respect of population growth. Rather, it has widened them, as revealed by the 2001 Census. For instance, Bihar recorded a much higher growth rate of population at 28.43 per cent during 1991-2001 as against 23.28 per cent in the previous decade.
Similarly, U.P recorded a higher population growth rate of 28.43 per cent against 23.38 per cent, and Haryana 28.6 per cent against 27.41 per cent. As against these States, Kerala recorded the lowest decadal population growth rate of 9.42 per cent followed by Tamilnadu of 11.19 per cent, Andhra Pradesh of 13.86 per cent and Karnataka of 17.25 per cent.
At the regional level, the South recorded the lowest decadal growth rate of population at 16 per cent, the West 40 per cent, the East 28 per cent and the North 30 per cent. The sex ratios also followed the same pattern in these regions.
6. Confined to Urban Areas:
The propaganda of family planning has been largely confined to urban areas and that too among the educated masses. Little has been done to propagate it in States where the birth rate is very high and the majority of population is illiterate and lives in villages. As a result, backward states like Bihar, U.P., Madhya Pradesh, and Orissa have remained almost unaffected by family planning programmes, as observed above.
7. Lack of Experienced Medical Personnel:
There have also been practical difficulties in the implementation of family welfare and child care programmes. Due to the lack of experienced doctors, nurses, midwives and other related staff, couples cannot be persuaded and their faith and trust cannot be won for the adoption of various family planning methods. Besides, even the quality of service has been poor. This has been one of the important factors for the failure of this programme.
8. Lack of Cheap Contraceptives:
There is the lack of cheap contraceptive methods in India which may be readily adopted by couples in the reproductive age group. Family planning surveys have revealed that the majority of couples in the reproductive age group do not want more children but are reluctant to use contraceptives.
9. Decline in Vesectomies:
There has been a steady and progressive decline in acceptors of vasectomy over the last decades. Presently, over 97 per cent of sterilisations are tubectomies of women.
Family Planning Programme for Population Control in India
India was the first country to evolve a government-backed family planning programme in the 1950s when the rest of the world was not aware of the problem. Today, after 47 years, India is trailing behind in population control. During the notorious Emergency regime between 1975 and 1977, the political leaders and many of their cronies, government officials and policemen shouted themselves hoarse advocating sterilization.
They devised ambitious programmes and carried them out against popular wishes and even used such harsh and coercive methods for sterilization that today one is reluctant to talk of family planning to the populace. The concerned officials have been scared away from it. The experts have jettisoned hopes of reaching the targets. In fact for all practical purposes, the country is without an effective programme or an effective target. Political parties studiously skirt the subject, and election campaigns are conducted without a word of it. What was once a highly dramatic political issue has suddenly become taboo.
In 1977, ‘family planning’ was rechristened as ‘family welfare’, and tasks beyond its competence embracing all aspects of family welfare, including improvement of women’s educational level, were included in it. In its family planning, awareness drive, the Government of India adopted the UNFP guideline of delaying the first child and spacing the subsequent birth(s).
The methods adopted in family planning are: sterilization, loop, pill, withdrawal, rhythm, sheath, and diaphragm. The condom and the pill seem most popular among the high socio-economic groups, the withdrawal method and the condoms among the middle socio-economic groups and sterilization is preferred by people belonging to the low social strata. Operations for family planning are not very popular among the socially well-placed, as this group is exposed to other methods of birth control. A good number of women use more than one method, depending on the circumstances, availability and the mood of the moment.
Measures Adopted:
Officially mobilized in 1951, only 147 family planning clinics were established during the First Five Year Plan period (1951-56). Since then, a network of Community Health Centres (CHCs), Primary Health Centres (PHCs), and Sub-Centres (SCs) has been created for implementing family planning programme through state governments with a hundred per cent central assistance. About 50,000 centres and sub-centres are created in rural areas in each Five Year Plan. In 1994, there were about 1.3 lakh SCs, 21,000 PHCs and 2,300 CHCs in the country (The Hindustan Times, July 11, 1995).
Of the various methods of family planning, the government till recently depended more on the ‘camp approach’ which relied implicitly on the district authorities applying pressure on their officials to intensify the sterilization campaign (mostly male sterilization). The government set targets for different states and districts and adopted persuasive, monetary, as well as coercive measures to achieve the targets. The highest rate of target achievement (190.9%) was in 1976-77 when the sterilization programme was ruthlessly and brutally implemented during the Emergency period.
The achievement rate of sterilization targets in different years has normally varied between 42 per cent and 64 per cent. The highest rate of achievement in 1976-77 has been described as ‘Sanjay Effect’ which was the result of coercion, cruelty, corruption, and inflated achievement figures. Sanjay Gandhi laid emphasis more on the sterilization method than on the 1UD (loop) method or conventional contraceptives (condoms).
The worst victims of cruelty and brutality of Sanjay Gandhi’s methods were the Harijans, peons, clerical staff, school teachers, innocent rural people, hospital patients, jail inmates and pavement-dwellers. This brutality through family planning (sterilization) method ultimately led to the fall of the government in 1977.
The Primary Health Centres in villages, engaged in family planning programmes, perform two specific functions: providing services to the people and disseminating information about these services in an effective manner in order to motivate the people to accept family planning. Nearly half a million medical and paramedical persons were engaged in the programme, besides half a million part-time village health guides.